Article Text

Abstract
Background Research documenting the relevance of neighbourhoods for the health of older adults has focused on global physical functioning outcomes, such as disability, rather than physiologic impairments that lead to disability. Muscle weakness is an age-related impairment and a central mechanism of disability. Evaluating neighbourhood effects on muscle weakness may offer insight into physiologic mechanisms of disability. We examined the association between perceived neighbourhood disorder and muscle strength in a nationally representative sample of US adults aged 51+.
Methods Among 11 277 participants (57% women; mean age: 66.6 years) in the Health and Retirement Study (2012–2014), we investigated whether self-reported neighbourhood physical disorder (1–7 scale, mean=2.61, SD=1.45); presence of vandalism/graffiti, litter, deserted houses, feeling safe walking alone) was associated with mean hand grip strength using linear regression models with sampling weights. We tested whether the association between neighbourhood disorder and grip strength differed by age and gender.
Results After adjusting for demographic characteristics, marital status, education and household wealth, residence in neighbourhoods with high perceived physical neighbourhood disorder was associated with lower muscle strength for men (β=−1.95 kg; 95% CI, 2.68 to –1.22) and to a lesser extent, for women (β=−0.64 kg, 95% CI, −1.11 to –0.19), (p for interaction <0.0001). For both men and women, associations between neighbourhood physical disorder and grip strength were more adverse among the middle aged (51–64 years) than for older (ages 65+) adults.
Discussion Perceived neighbourhood disorder was associated with lower muscle strength. Future studies should more rigorously evaluate causality and evaluate potential interventions.
- epidemiology of ageing
- functioning and disability
- neighbourhood/place
- social epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Neighbourhoods predict functional limitations and disability1–4; however, the physiologic mechanisms underlying these associations remain poorly understood. Disability in older adults reflects the consequences of physiologic impairments such as muscle weakness, environmental demands and opportunities for accommodation. Evaluating whether neighbourhoods influence physical impairments per se would help understand how neighbourhoods shape disability and pinpoint potential interventions. Half of US older adults meet clinical criteria for muscle weakness5 and muscle weakness increases both cardiovascular6 and all-cause mortality.7 8 To date however, there is little evidence on social or contextual determinants of muscle weakness. Examining the role of neighbourhood environment in relation to muscle weakness represents an unexplored mechanism linking neighbourhoods and disability.
The social and economic conditions of residential neighbourhoods predict many health domains among older adults and could plausibly affect muscle weakness.9 For example, neighbourhood crime is associated with physical inactivity and obesity.10 A reduction in neighbourhood disorder is related to improved physical activity levels, increased recovery from mobility limitation and lower risk of subsequent disability in older adults.10–12 Residents of neighbourhoods with lower average socioeconomic position are at greater risk for deficits in physical functioning and disability.10 Therefore, clarifying the relationship between the social neighbourhood environment and muscle strength may offer a deeper understanding into how neighbourhoods influence physical functioning and disability while providing novel insights into the underlying physiologic mechanisms underlying the previously observed neighbourhood-disability association.
Neighbourhood physical disorder, defined as visible signs of neglect and/or decay, such as an increased presence of crime, graffiti litter/garbage and the number of vacant homes,13 14 is a key component of the social neighbourhood environment that may have indirect consequences for muscle strength. Several studies have found that when residents perceive their environment as unsafe or threatening, they may be less likely to leave the house, making outdoor walking and engaging in physical activity more difficult due to increased fears of victimisation and reduced physical safety.11 12 15 As a result, given existing evidence that physical activity has positive benefits for muscle strength among older adults,16 17 increased exposure to neighbourhood physical disorder may serve as barrier, leading to an indirect decrease in muscle strength, particularly among older adults.
Based on the earlier point, we hypothesised that greater perceived neighbourhood physical disorder would be associated with lower muscle strength in a nationally representative sample of adults aged 51 years and older. Specifically, we hypothesised that compared with individuals residing in neighbourhoods with the lowest neighbourhood physical disorder, individuals who reported exposure to moderate or high levels of perceived physical neighbourhood disorder would have decreased muscle strength, even after adjusting for known confounders. We also hypothesised that this association may be modified by age whereby older individuals (65+) who reside in neighbourhoods with greater physical disorder would have lower muscle strength compared with younger individuals (51-64).
Methods
Study design and sample population
The Health and Retirement Study (HRS) is a nationally representative, multistage area probability survey of non-institutionalised, community dwelling Americans aged 51 years and older. Study details have been previously described.18 Sampled persons have been re-interviewed biannually since 1992, and new cohorts have been added to the original sample to maintain the nationally representative nature of the survey over time.18
Starting in 2006, a half sample of HRS participants were randomly selected for an enhanced face-to-face interview that included physical measurements, and the other random one-half completed the same interview in 2008.19 In addition, in the same 2006 survey wave, HRS began collecting data on psychological and social well-being that was left behind after the enhanced face-to-face interview and respondents were surveyed every 4 years.20 Participants completed these questions and then mailed in their responses. For this analysis, we used two waves of data from the 2012 and 2014 surveys to create one cross-sectional wave (2012/2014).
Our initial population included 21 226 individuals who were 51+years old in 2012/2014. Individuals who had died (n=1245), were in a nursing home, not cohort eligible, non-interviews or not interviewed in that wave (n=3479) were also excluded. Individuals who were missing data on the exposure variable due to feeling unsafe, refused or tried but were unable to complete the physical measurement assessment were excluded (n=2065) while those who did not have exposure data due to not returning the mail-in enhanced face-to-face questionnaire were excluded (n=2784). Individuals who were also missing on grip strength (n=376) were also excluded, yielding a final analytic sample of n=11 277 men and women.
Measures
Outcome: hand grip strength
Our primary outcome of interest was hand grip strength, which was assessed using a Smedley spring-type hand dynamometer (Scandidact). Participants were instructed to squeeze the device with the dominant hand as hard as they could and then let go. Grip strength assessments were administered while participants were standing with their arm at their side, and with the elbow flexed at a 90 degree angle.19 After one practice trial, two measurements were taken with each hand, alternating hands. The maximum measurement in kilograms from the four trials was used for the analysis.
Exposure: perceived neighbourhood physical disorder
Our primary exposure of interest was perceived physical neighbourhood disorder. Respondents were asked to assess physical neighbourhood disorder based on four indicators: presence of (1) vandalism/graffiti, (2) rubbish/litter, (3) vacant/deserted homes and (4) crime. Respondents rated their perceptions of their local neighbourhood, defined as ‘everywhere within a 20 min walk or about a mile’ of where they lived on a 7-point Likert scale. The perceived neighbourhood physical disorder was created by averaging the scores of the four disorder items, with higher scores indicating more physical disorder. Respondents with two or more missing items (of the four items) were recoded as missing for the final averaged score. We created tertiles of neighbourhood physical disorder since the continuous variable was not normally distributed with individuals residing in no/low, moderate and high disorder neighbourhoods although alternative conceptualisations (binary, quartiles) also yielded similar results. The physical neighbourhood disorder scale was adapted from the Project on Human Development in Chicago Neighborhoods13 and the Cronbach’s alpha was 0.83 and 0.84 in 2012 and 2014, respectively.20
Covariates
The following hypothesised confounders were included in our models: age (continuous), self-reported race/ethnicity (Black, White and Other), education (3-level categorical variable; less than a high school degree, high school degree, some college/college degree), marital status (3-level categorical variable; married/partnered, separated/divorced/widowed and single/never married), and household wealth, a continuous measure, defined as the net value of total wealth calculated as the sum of all wealth components less all debt. In order to account for household size relative to household wealth, we divided the average household wealth by the square root of the number of household members.
Analytic strategy
Differences in demographic characteristics between men and women who resided in no/low, moderate and high perceived neighbourhood disorder were assessed using Statistical Analysis System (SAS) survey procedures based on t-tests for continuous variables and Rao χ2 tests for categorical variables. Descriptive analyses were weighted using HRS sampling weights to account for non-response and the complex survey design. A model building strategy was employed: first we adjusted for age then added demographic characteristics such as race/ethnicity, marital status and education and finally, for household wealth. We also tested two interaction terms. First, due to known differences in grip strength by gender,21 an interaction term between neighbourhood disorder and gender examined whether the association between disorder and strength differed by men and women. Second, an age × neighbourhood interaction term tested the hypothesis that the neighbourhood environment may be more consequential for grip strength among those who are older (65+ years, n=6596) vs younger (<65 years old, n=4681). To increase statistical power, we also entered a continuous age × neighbourhood term into the model. We proceeded with gender-stratified, weighted linear regression models to estimate the association between categorical neighbourhood physical disorder (low, moderate and high) and mean maximum hand grip strength (kg). We present 95% CIs for coefficients and statistical significance for interactions was assessed with a two-tailed alpha of p value<0.05. All analyses were conducted using SAS V.9.4.22
Results
Tables 1 and 2 present the weighted descriptive statistics for men (n=4780) and women (n=6873), respectively, from 2012 to 2014 HRS. We present results separately for men and women due to known differences in hand grip strength and after testing an interaction term, which indicated that greater neighbourhood disorder was associated with higher grip strength among men compared with women (p for interaction<0.0001).
Descriptive statistics for 4692 men in the HRS (2012–2014)
Linear regression coefficients for neighbourhood physical disorder predicting muscle strength in 4692 men in the HRS (2012–2014)
Results for men
Among men (table 1), mean hand grip strength was 41 kg. On average, men who resided in neighbourhoods with higher neighbourhood disorder had slightly lower mean hand grip strength, higher body mass index (BMI), lower reported levels of moderate physical activity, greater self-reported depression levels and a higher number of chronic conditions (all p<0.0001).
In age-adjusted models (table 2, Model A), compared with men who resided in neighbourhoods with no/low perceived physical disorder, men who reported moderate (β=−1.13 kg, 95% CI, −1.85 to –0.40) and high (β=−3.25 kg, 95% CI, −3.94 to –2.47) levels of disorder had lower muscle strength. Results were similar but slightly attenuated after adjusting for demographic characteristics (Model B). In the fully adjusted model controlling for household wealth (Model C), compared with men residing in neighbourhoods with no/low neighbourhood physical disorder, men in high disorder neighbourhoods had, on average, hand grip strength that was about 2 kg lower (β=−1.95, 95% CI, −2.68 to –1.22).
Results for women
The mean overall hand grip strength for women was 25 kg (table 3). Women residing in neighbourhoods with greater perceived physical disorder had slightly lower muscle strength (p<0.0001). Among women living in neighbourhoods characterised by greater perceived neighbourhood physical disorder, there were, on average, higher self-reported levels of depression, lower levels of physical activity, higher number of chronic conditions and greater BMI levels (all p<0.0001).
Descriptive statistics for 6585 women in the HRS (2012–2014).
In age adjusted models for women (table 4, Model A), living in neighbourhoods with moderate (β=−0.30, 95% CI, −0.75 to 0.15) or high (β=−0.87, 95% CI, −1.33 to –0.43) perceived physical disorder was associated with slightly lower muscle strength compared with living in no/low disorder neighbourhoods. Adjusting for race/ethnicity, marital status and education only slightly attenuated the association (Model B). In the fully adjusted wealth model (Model C), women residing in neighbourhoods with high perceived neighbourhood physical disorder had lower grip strength compared with those living in neighbourhoods with no/low disorder (β=−0.65, 95% CI, −1.11 to –0.19).
Weighted linear regression model examining the association between neighbourhood physical disorder and muscle strength in 6585 women in the HRS (2012–2014)
Results for interaction models
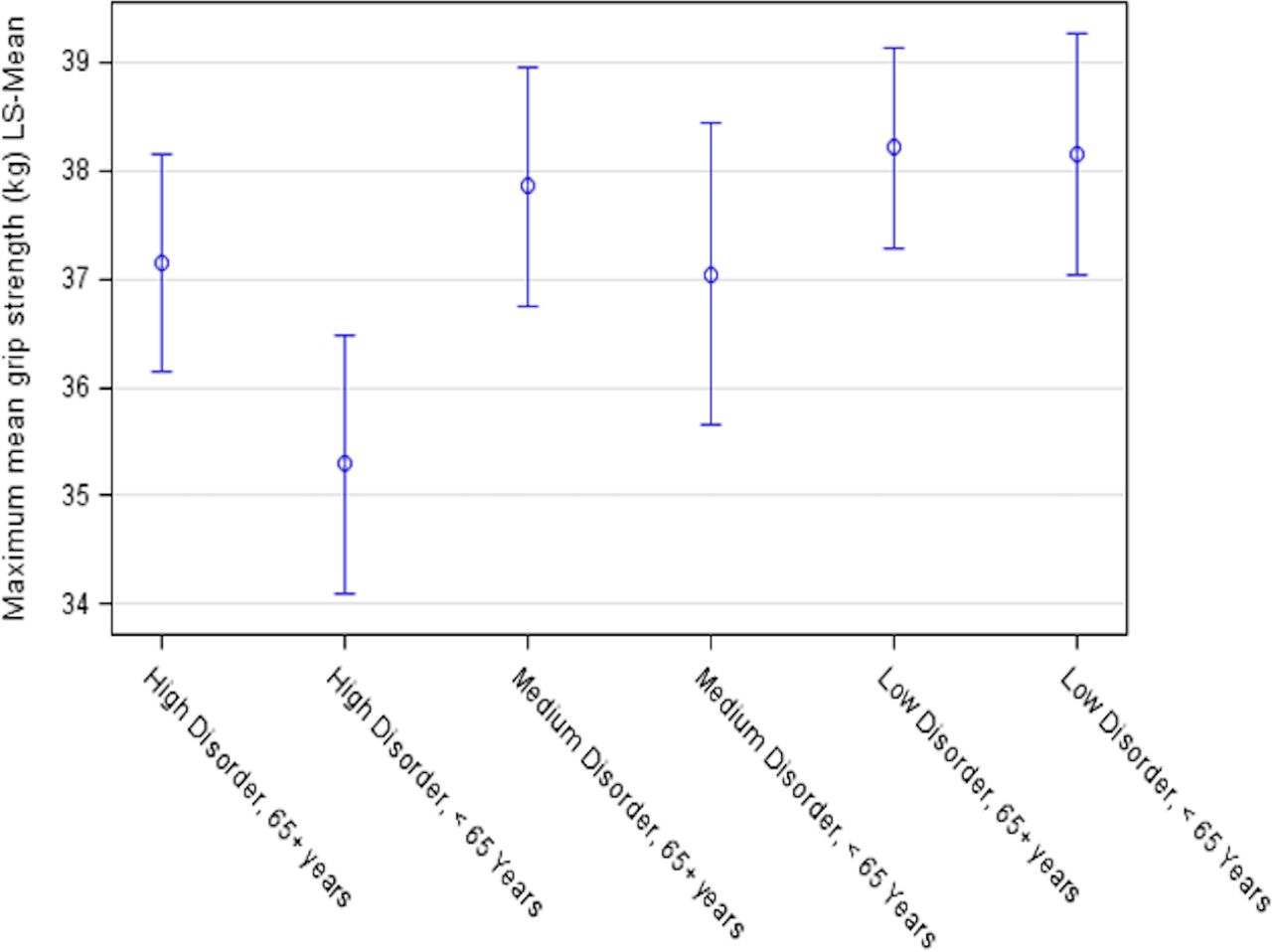
We tested the hypothesis that neighbourhood disorder and muscle strength might differ among the middle aged (51–64 years) and older adults (65+years). We observed a significant interaction between neighbourhood disorder and age with the mean level of grip strength (p<0.01). Specifically, among men, the association of neighbourhood physical disorder was more adverse for the middle aged compared with older adults. Middle-aged men residing in neighbourhoods with no/low physical disorder had a predicted grip strength of 38.2 kg while those residing in neighbourhoods with high perceived disorder had a mean level grip strength of 45.3 kg—a 3 kg difference ( β =1.79, 95% CI, 0.53 to 3.06). Among older adults, men residing in neighbourhoods with high disorder had a predicted grip strength that was 1 kg lower compared with men living in neighbourhoods with the lowest disorder (p<0.01) (see online supplementary file 1, table 1, Model D). Among women, there was no evidence that neighbourhood disorder and grip strength differed by age (p=0.14) (figures 1 and 2) (supplement, table 2, Model D). Similar interaction results were also observed using the continuous age interaction term for both men and women (see online supplementary file 1, tables 1 and 2, Model E, respectively) for the age × neighbourhood disorder models.
Supplemental material

Predicted mean grip strength by level of perceived neighbourhood disorder and age among men in the health and retirement study (2012/2014).

{kind=link}
{kind=link}
Predicted mean grip strength by level of perceived neighbourhood disorder and age among women in the health and retirement study (2012/2014).
Discussion
In this nationally representative sample of adult men and women aged 51+ years, greater perceived neighbourhood physical disorder was associated with lower hand grip strength, a valid surrogate of total body muscle strength.6 The association was stronger for men than for women and stronger for middle-aged adults than older adults. The results of this study indicate the social environment may affect muscle strength. Our findings of gender differences are consistent with previous research indicating that men may be more influenced by their neighbourhood environment. For example, neighbourhood walkability was inversely related to depressive symptoms in 740 adults in King County, Washington among men, but not women.23
We initially hypothesised that older adults may be more vulnerable to the health-promoting or health-damaging aspects of residential neighbourhoods as they may be more likely to depend on local resources to maintain quality of life and be emotionally invested in their community.24 Our results, however, indicate that physical disorder was more consequential for middle-aged men than older adult men. Middle-aged adults are more likely to be physically active compared with older adults.25 It is possible that higher levels of perceived disorder may serve as a greater barrier for this age group than for older adults who may have already begun to reduce their physical activity levels and restrict their life space.26
Muscle weakness may serve as a key mechanism linking the neighbourhood environment with physical functioning, frailty and disability,2 27–29 although more research is needed to fully evaluate these relationships. There are several pathways by which neighbourhood disorder could ‘get under the skin’ to influence muscle strength, including activation of stress response.15 Individuals who reside in neighbourhoods with higher levels of neighbourhood disorder may experience chronic activation of the stress response, which has implications for muscle health. Repeated activation of the hypothalamic–pituitary–adrenal pathway causes hypersecretion of cortisol, which has been found to be independently linked to poorer physical performance, including muscle strength.30 31 For example, in one longitudinal study of 1200 older adults, higher cortisol levels were associated with higher risk of loss of grip strength over a 4-year period.32 In addition, when residents perceive their environment as unsafe or threatening, they may be less likely to leave the house, making outdoor walking and engaging in physical activity less appealing and accessible.12 15 33 Given known evidence that physical activity increases muscle strength,34 higher levels of neighbourhood disorder may lead to behavioural changes that indirectly decrease muscle strength.
While the overall effect sizes observed in this study were small, they nonetheless may be important. Prior work investigating the minimum clinically important difference (MCID) in grip strength levels in a longitudinal setting found that, on average, a change in grip strength of ~6 kg may be a MCID.35 In our study, men residing in neighbourhoods with the highest level of disorder had hand grip strength on average 2 kg lower compared with men residing in the lowest levels of disorder; this was equivalent to about a 4-year age difference. For women, the absolute difference between highest and lowest levels of disorder was about 0.6 kg, roughly equivalent to a 3-year age difference. Since more than half of all men and women in our sample report being exposed to moderate or high levels of physical disorder in their community of residence, these results may translate into large population-level effects.
This study has several important limitations. First, given the cross-sectional design of this study, temporal ordering cannot be established. Weaker (or sicker) individuals may be more likely to move into neighbourhoods with greater disorder, that is, reverse causation. Second, we were unable to test specific mechanisms of the neighbourhood disorder–strength association. Future research should explore the role of increased levels of cortisol or other possible physiologic mechanisms. Third, given the progressive and dynamic nature of ageing, using a dichotomous age variable (65+ vs <65 years) to compare older to younger adults is somewhat arbitrary. However, we chose this threshold to both illustrate the magnitude of the difference and based on previous work investigating the influence of neighbourhoods on older adults.1 4 35 Finally, we used a self-reported measure of neighbourhood disorder. This may pose a threat to internal validity if weaker individuals were more likely to report higher levels of disorder. Nonetheless, it is unclear why muscle strength would influence perceived neighbourhood disorder. Other studies have found this same measure of perceived physical disorder to be an important predictor of other health outcomes, including disability recovery, physical functioning and insomnia.14 35 36
Despite these limitations, this study has several strengths. Most importantly, this study addresses a major gap in research on muscle weakness: an evaluation of the role of social determinants such as the residential neighbourhood environment. Further, we help fill in understanding of why neighbourhoods may influence disability, showing a specific physiologic mechanism. This is a first study in this domain, and results justify longitudinal analyses with formal causal mediation methods. In a field focused on clinical risk factors, social determinants offer an unrealised opportunity to improve muscle strength and thereby improve functioning and independence of middle aged and older adults. Policies and interventions can change physical disorder in communities. Finally, policies and interventions can be developed to deliver resources to middle-aged individuals, living in communities with high levels of disorder, in order to offset the effects of such disorder.
In summary, in this nationally representative sample of men and women, higher levels of neighbourhood disorder were associated with lower muscle strength, and this observed relationship was stronger for men than for women. To the best of our knowledge, this is the first study to demonstrate a relationship between perceived neighbourhood disorder and muscle strength using nationally representative data of adults aged 51+ years. Future studies should more rigorously evaluate causality and evaluate whether interventions that improve the neighbourhood environment also affect muscle strength.
What is already known on this subject
Neighbourhoods predict functional limitations and disability; however the physiologic mechanisms underlying these associations remain poorly understood.
The social neighbourhood environment predicts many health domains among older adults and could plausibly affect muscle weakness.
Several studies have found that when residents perceive their environment as unsafe or threatening, they may be less likely to leave the house, making outdoor walking and engaging in physical activity more difficult due to increased fears of victimisation and reduced physical safety.
What this study adds
In a nationally representative sample of older adults aged 51+ years, greater perceived neighbourhood physical disorder was associated with lower hand grip strength, a valid surrogate of total body muscle strength. The association was stronger for men than for women and stronger for middle-aged adults than older adults.
This study helps to fill in understanding of why neighbourhoods may influence disability, showing a specific physiologic mechanism.
The neighbourhood environment offers an unrealised opportunity to improve muscle strength and thereby improve functioning and independence of middle-aged adults and older adults.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @cadkat
Contributors KAD drafted the conceptual model, manuscript and completed the statistical analyses. MMG and PMC provided feedback on the conceptual model, assisted with the interpretation of the data and provided critical review of the manuscript.
Funding This research was supported by the National Institute on Aging of the National Institutes of Health under Award T32-AG049663.
Competing interests PMC reports consultation to BioAge Labs, and grants to her institution from Abbott and Nestle, all for work outside of this project.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are from the health and retirement study and can be accessed at https://hrs.isr.umich.edu.