Article Text

Abstract
Background Socioeconomic inequalities in child vaccination continue to be a global public health concern. This study aimed to measure and identify factors associated with socioeconomic inequalities in full immunisation coverage against the four core vaccine-preventable diseases (ie, bacille Calmette-Guérin, diphtheria-tetanus-pertussis (three doses), polio (three doses) and measles vaccines) in 46 low/middle-income countries.
Methods The most recent nationally representative samples of children (aged 10–59 months, n=372 499) collected through the Demographic Health Surveys were used to measure vaccination rates. The concentration index (C) was used to quantify socioeconomic inequalities in vaccination coverage. Furthermore, meta-regression analyses were used to determine factors affecting socioeconomic inequalities in vaccination coverage across countries.
Results Results suggested that immunisation coverage was pro-rich in most countries (median C=0.161, IQR 0.131). Gambia (C=−0.146, 95% CI −0.223 to −0.069), Namibia (C=−0.093, 95% CI −0.145 to −0.041) and Kyrgyz Republic (C=−0.227, 95% CI −0.304 to −0.15) were the only countries where children who belong to higher socioeconomic status group were less likely to receive all the four core vaccines than their lower socioeconomic status counterparts. Meta-regression analyses suggested that, across countries, the concentration of antenatal care visits among wealthier mothers was positively associated with the concentration of vaccination coverage among wealthier children (coefficient=0.606, 95% CI 0.301 to 0.911).
Conclusions Pro-rich distribution of child vaccination in most low/middle-income countries remains an important public health policy concern. Policies aimed to improve antenatal care visits among mothers in lower socioeconomic groups may mitigate socioeconomic inequalities in vaccination coverage in low/middle-income countries.
- Socioeconomic inequalities
- child vaccination
- developing countries
Statistics from Altmetric.com
Introduction
In spite of the remarkable global improvement in routine vaccination coverage worldwide, the overall improvement is not equally distributed among the countries.1 Furthermore, a growing body of evidence suggests that there exists a social gradient in child vaccination within countries. For example, children whose parents are well-educated, wealthy or living in urban areas have a higher probability to be immunised against vaccine-preventable diseases.2 3 Social inequalities in vaccination uptake can potentially hinder the global efforts to reduce the burden of disease in low/middle-income countries because children from socioeconomically disadvantaged backgrounds are generally at increased risk of contracting infectious diseases.4
Incomplete or complete lack of vaccination remains the cause of millions of preventable child deaths each year in low/middle-income countries; there is, therefore, a considerable amount of literature devoted to factors that impact vaccination uptake. Although several studies (eg, refs 5–9) suggest that socioeconomic inequalities are still a major barrier to child immunisation in low/middle-income countries, few studies (eg, ref 10) aimed to quantify socioeconomic inequalities in vaccination coverage using a summary measure of inequality such as the concentration index. Measuring and monitoring of socioeconomic-related inequalities in child vaccination in low/middle-income countries play a major role in evaluating progress towards the targets made by national and international programmes to improve child vaccination coverage. Identifying factors that explain the concentration of incomplete child vaccination among lower socioeconomic status (SES) children can also provide valuable information to introduce effective strategies and policies to address such inequalities.
Using the most recent nationally representative samples of children collected through the Demographic Health Surveys (DHS) and the concentration index approach (which accounts for inequality across the whole socioeconomic distribution), this study aimed to measure socioeconomic inequalities in full immunisation coverage against the four core vaccine-preventable diseases (ie, bacille Calmette-Guérin (BCG), diphtheria-tetanus-pertussis (DTP, three doses), polio (three doses) and measles vaccines, see online supplementary table 1) in 46 low/middle-income countries. Additionally, meta-regression analyses were performed to examine whether inequalities in proximate determinants of child vaccination were associated with the extent of socioeconomic inequality in vaccination across countries.
Supplemental material
Methods
Data
The data for this study were obtained from the Standard DHS from 46 low/middle-income countries collected through the MEASURE DHS project over the period between 2010 and 2015. The DHS surveys are nationally representative cross-sectional household surveys with large sample sizes, typically between 5000 and 30 000 households.11 Using a multistage sampling procedure,12 the DHS collects reliable and comparable information on a variety of health-related topics13 such as vaccination status of children in the household. High response rates and national coverage are key advantages of the DHS.14 To facilitate comparability of surveys across time and countries a similar set of questions is used.13 Data collection methods, validation and reliability assessment are described elsewhere.13 Immunisation records of children aged 59 months and younger were drawn from the DHS surveys. To allow each child a follow-up period to receive all the four routinely recommended core vaccines: BCG, DTP (three doses), polio (three doses) and measles vaccines (10 months as per the WHO15 recommended immunisation schedules for the four routine vaccines, see online supplementary table 1), 82 694 live births that occurred less than 10 months before the survey interview were excluded from the analysis. The final sample contained 372 499 live births aged 10–59 months in 46 low/middle-income countries between 2010 and 2015. Online supplementary table 2 presents the survey years, sample size and gross national income (GNI) per capita (current US$) for the sampled countries.
Measures
The outcome variable in this study is binary variable indicating whether a child received all the four routinely recommended core vaccines. Immunisation status of children was collected using vaccination record cards provided by mothers or caregivers during the survey interview. In the absence of vaccination cards, mothers’ or caregiver’s verbal reports of children’s immunisation coverage were used. Maternal reports may suffer from recall bias; however, previous studies (eg, ref 16) showed that maternal recall reports are valid when we compare child vaccination coverage across populations. Socioeconomic inequalities in vaccination coverage among children were measured using a constructed wealth index (WI) for each household in the DHS surveys as a measure of child SES. Using a principal components analysis (PCA) technique the DHS uses information on selected household’s assets to construct the WI.17 Based on the extant literature (eg, refs 5 6), the effects of inequalities in income and other proximate determinants of vaccination uptake (which have been consistently collected in all DHS surveys) on socioeconomic inequalities in vaccination coverage were assessed. This included socioeconomic inequalities in mother’s education, mother’s age 19 and below, higher number of children under 5 in the household (3 and above) and antenatal care (ANC) coverage (a minimum of four prenatal care visits), and income inequality as measured by Gini index. As the DHS does not collect information on expenditure or income, the World Bank’s World Development Indicators and Global Development Finance data set18 was used to obtain Gini index for each country in the study.
Statistical analysis
The statistical analysis involved two steps: (1) calculating socioeconomic inequalities in vaccination coverage and (2) performing meta-regression analyses to determine factors affecting socioeconomic inequalities in vaccination coverage.
Measuring socioeconomic inequalities
Socioeconomic inequality in vaccination coverage in each country was measured using the (relative) concentration (C) index. The C index is measured regarding the (relative) concentration curve, which plots the cumulative share of vaccination coverage, on its y-axis, against the cumulative share of the children, ranked in ascending order of SES (WI), on its x-axis. If all children, ranked by WI, received an equal proportion of vaccination coverage, the curve would coincide with the 45° line (ie, the line of ‘perfect equality’). The C index is described as twice the area between the 45° line and the concentration curve. The C index ranges from −1 to +1, with zero representing ‘perfect equality’.19 If a health variable is concentrated among the rich, multiplying the C index by 75 will give us the fraction of health variable that needs to be transferred from the wealthier half to the poorer half to achieve ‘perfect equality’.20
The C index can be computed using the ‘convenient regression’ approach as follows21:
 (1)
(1)
where  is child
i
’s vaccination coverage status, μ is the mean of vaccination coverage for the total sample,
is child
i
’s vaccination coverage status, μ is the mean of vaccination coverage for the total sample,  is the fractional rank of child
i
in the distribution (
is the fractional rank of child
i
in the distribution ( and
n
for the poorest and wealthiest child, correspondingly), and
and
n
for the poorest and wealthiest child, correspondingly), and  indicates the variance of fractional rank. The ordinary least squares (OLS) estimate of
β
represents the C index and its SE provides the SE for the C index.22 As the outcome variable in this study is binary, the C index was normalised23 to summarise wealth-related inequalities in vaccination coverage by multiplying by
indicates the variance of fractional rank. The ordinary least squares (OLS) estimate of
β
represents the C index and its SE provides the SE for the C index.22 As the outcome variable in this study is binary, the C index was normalised23 to summarise wealth-related inequalities in vaccination coverage by multiplying by  . To obtain estimates that are representative of children (aged 10–59 months) living in each country sampling weights were applied in the calculation of the C index. 95% CIs were used to assess statistical significance of the C index. A method suggested by Altman and Bland24 was used to examine the significance of differences in the C at 95% CI.
. To obtain estimates that are representative of children (aged 10–59 months) living in each country sampling weights were applied in the calculation of the C index. 95% CIs were used to assess statistical significance of the C index. A method suggested by Altman and Bland24 was used to examine the significance of differences in the C at 95% CI.
Meta-regression analyses
Univariate and multivariate meta-regression analyses were performed to assess the determinants of socioeconomic inequalities in vaccination coverage. The C index in vaccination coverage for each country was used as the dependent variable and socioeconomic inequalities in proximate determinants of vaccination uptake (measured by the C index) and income inequality (measured by the Gini index) were used as explanatory variables. The number of covariates in the model satisfies the ‘rule of thumb’ of having at least 5–10 observations per predictor in multivariable regression analysis.25 The random effects models were used in the meta-regression analyses. This is because fixed effects meta-regression assumes that the covariates included in the model can explain all the heterogeneity in the outcome variable and thus is not often recommended.26 The inverse variances of the C index for vaccination coverage were used as weights in all univariate and multivariate meta-regression analyses. All analyses were performed in V.13 of the STATA software package (StataCorp, College Station, Texas).
Results
Child vaccination coverage
Online supplementary table 3 and figure 1 present the percentage of children (aged 10–59 months) who received all the four core vaccines in 46 low/middle-income countries. Overall, 55.5% of children in the sampled countries were immunised against the diseases. There was a significant difference across the countries in the vaccination uptake; for example, in Nepal, Honduras and Armenia more than 85% of children received all the four vaccines, whereas this figure was less than 35% in Mali, Nigeria and Ethiopia. As reported in online supplementary table 3, up to 58.3% of children in low-income countries completed immunisation for the four main diseases; these figures were 52.9% and 68% in the sampled lower middle-income and upper middle-income countries, respectively.

Child vaccination coverage (%) against the four core vaccine-preventable diseases in 46 low/middle-income countries.
As reported in online supplementary table 3, the vaccination rates were generally similar for males and females in all countries, except Gambia, Tanzania, Honduras and Gabon, where vaccination uptakes were slightly higher among men compared with women. The results also indicated that child vaccination was higher in urban areas compared with rural areas in most countries. The vaccination rates were significantly higher in rural than urban areas in Gambia, Namibia, Kyrgyz Republic, Malawi and Honduras.
Socioeconomic inequalities in child vaccination coverage
Table 1 reports the magnitude of socioeconomic inequalities in immunisation coverage in 46 low/middle-income countries. The results suggested that immunisation coverage is pro-rich in the majority of countries (median C=0.161, IQR 0.131). Gambia (C=−0.146, 95% CI −0.223 to −0.069), Namibia (C=−0.093, 95% CI −0.145 to −0.041) and Kyrgyz Republic (C=−0.227, 95% CI −0.304 to −0.15) were the only countries where children who belong to higher SES were less immunised compared with lower SES counterparts. As shown in figure 2, socioeconomic inequalities in vaccination coverage were higher in countries such as Nigeria, Pakistan, Yemen, Cambodia, Cameroon and Indonesia compared with the other countries. The results did not suggest any association between socioeconomic inequalities in immunisation coverage and (log) GNI per capita (r(44)=−0.020, p=0.89).
Socioeconomic inequalities in child vaccination coverage in 46 low/middle-income countries

Socioeconomic inequalities in child vaccination coverage and gross national income (GNI) per capital (current US$) in 46 low/middle-income countries.
The C index indicated persistent pro-rich inequalities in vaccination coverage in urban (median C=0.154, IQR 0.141) and rural areas (median C=0.163, IQR 0.171) in most of the sampled countries. Peru and Togo were the two countries with the pro-poor distribution of child immunisation in rural areas. While in countries such as Nigeria, Pakistan, Gabon and Jordan socioeconomic inequalities were significantly higher in rural compared with urban areas, in countries such as Ethiopia, Togo, Peru and Nepal socioeconomic inequalities in vaccination uptake were greater in urban compared with rural areas.
Factors affecting socioeconomic inequalities in child vaccination coverage
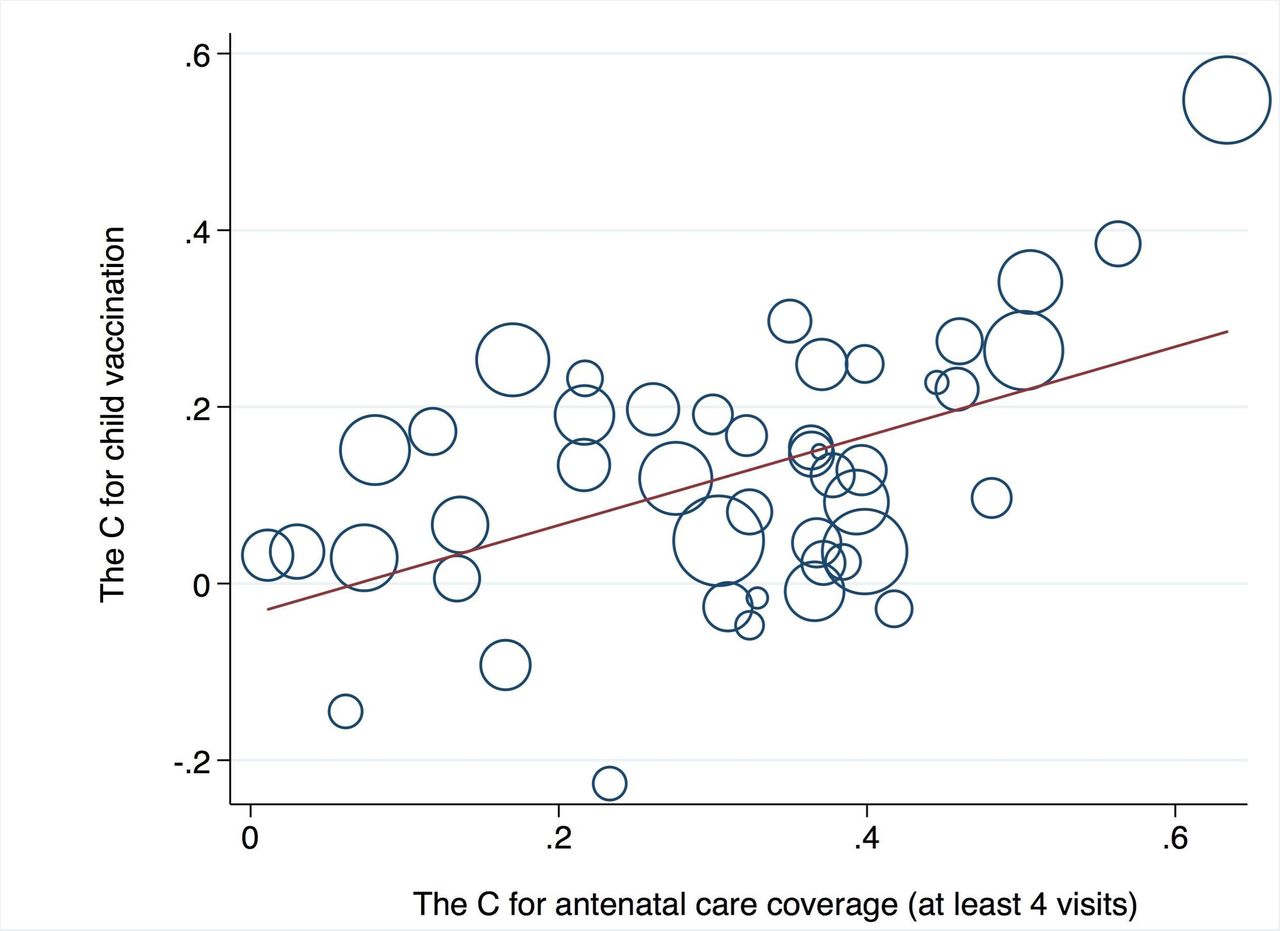
Table 2 reports the meta-regression analysis results. According to the univariate meta-regression results, the concentration of mother’s educational level (coefficient=0.361, 95% CI 0.091 to 0.63) and ANC coverage (coefficient=0.505, 95% CI 0.248 to 0.762) among wealthier children was positively associated with socioeconomic inequalities in vaccination coverage. In multivariate analysis, only the concentration of ANC use among wealthier women was associated with socioeconomic inequalities in vaccination coverage; a 10% increase in the magnitude of the C index for ANC use was associated with a 6% increase in the value of the C index for vaccination coverage. Figure 3 demonstrates bubble plots of the correlations between the C index for mother’s ANC use and the C index for vaccination coverage.
Meta-regression analysis results
{kind=link}
{kind=link}
{kind=link}
Bubble plot of the association between the C indices for child vaccination and antenatal care coverage (at least four visits). The size of the bubbles in the figure is proportional to the weight of each observation in the meta-regression analysis.
Discussion and conclusions
This study, similar to previous studies in low/middle-income countries (eg, refs 5–8), found pro-rich inequalities in immunisation rate in most countries under study. Gambia, Namibia and Kyrgyz Republic were the only countries where children who belong to higher SES households were less likely to be fully immunised against the four diseases than their lower SES counterparts. Lower vaccination coverage among higher versus lower SES children was also observed in more developed countries (eg, ref 27). Studies27–29 have suggested several factors that may be associated with a decrease in child vaccination coverage among higher SES population in more developed countries. The significant reductions in the incidences of vaccine-preventable diseases in recent decades may have changed how parents perceive child vaccines. In other words, parents may perceive fewer benefits associated with vaccines than the risks of rare adverse events following immunisation. Some scientifically unfounded claims about vaccines that link some vaccines to problems such as autism, multiple sclerosis, sudden infant death syndrome and other problems may have also altered the perception of the usefulness of vaccines in some developed countries. Although these factors may explain pro-rich inequalities in child vaccinations in more developed countries, additional investigations are required to further elucidate this issue in low/middle-income countries.
The finding from univariate meta-regression demonstrated that the concentration of educational attainment among mothers who belong to higher SES household was positively associated with the pro-rich distribution of child immunisation. The impact of unequal distribution of maternal education on inequality in child vaccination uptake can be explained through human, social, cultural and empowerment routes. The human capital advantage of maternal education in higher compared with lower SES households can lead to greater receptivity to public health messages aimed at boosting child immunisation rates among higher SES household because highly educated mothers have a greater understanding about the benefits of immunisation.30 Educated mothers also have larger social networks (social capital) which provide good health behaviour-related information and where to find available healthcare services. The social capital of well-educated mothers can result in higher concentration of immunisation rates among children from wealthier households. Moreover, well-educated mothers generally have socially valued general skills that provide them with a higher social status. This cultural capital can result in better communications between mothers and medical providers and thus enables wealthier households to use more healthcare such as immunisation services.31 Higher educational attainment (as a means for empowering women) among wealthier mothers also assists them to play an active role in public and in their households which enables them to insist on better healthcare (eg, vaccination coverage) for their newborn babies.32
Results of both univariate and multivariate meta-regression analyses suggested that, across countries, the concentration of ANC among wealthier mothers was statistically significantly positively associated with the concentration of vaccination coverage among wealthier children. Previous studies (eg, refs 33 34) have documented the positive impact of ANC visits on child vaccination coverage. The positive impacts of pro-rich inequalities in ANC visits on the concentration of child vaccination coverage can be attributed to the fact that higher compared with lower SES mothers have more opportunities to receive messages about the benefits of child vaccination that encourage them to use vaccination services for their newborns because they use more ANC services. ANC visits establish communication and build trust between healthcare providers and mothers, which, in turn, may affect mothers’ immunisation-seeking behaviours.35 By increasing the interaction between health personnel and mother, ANC care visits can address some of the reasons behind low rate of vaccine uptake, including lack of information about immunisation benefits, fear of side effects and unfamiliarity with place and time of immunisation.36
Methodological overviews of measuring and monitoring inequalities in health recommend reporting both absolute and relative measures to ensure appropriate tracking of health inequalities.37 Thus, a modified absolute (generalised) concentration (AC) index38 was used to compute and identify key determinants of absolute socioeconomic inequalities in vaccination coverage across the sampled countries. More information about the AC index can be found elsewhere.38 39 The results were qualitatively very similar to those obtained using the C index to measure socioeconomic inequalities (see online supplementary tables 4 and 5 and supplementary figures 1 and 2). The results of multivariate meta-regression analysis using the AC index suggested that, across countries, the concentration of ANC and educational attainment among wealthier mothers was statistically significantly positively associated with the concentration of vaccination coverage among wealthier children. Furthermore, similar to the results obtained from multivariate meta-regression analysis using the C index, the concentration of the presence of three or more siblings (aged <5 years) in the household among the poor households had a positive effect on absolute socioeconomic inequality in immunisation coverage. This latter result can be explained by the fact that the concentration of larger numbers of children in poor households encompasses a greater competing demand for mothers’ limited time and resources resulting in lower rates of immunisation among the poor children.40
This study is subject to some limitations. First, similar to other studies using DHS data sets to determine factors associated with child vaccination,6 maternal recall was used to identify the child’s vaccination status in the absence of vaccination record card. Although the validity of relying on maternal recall to obtain child’s vaccination status has been confirmed,16 it would be ideal to use a written record to obtain this information to avoid potential recall bias. Second, as the DHS collects vaccination coverage of still living children at the time of the survey interview, this study indicates socioeconomic inequalities in vaccination coverage among children who were alive at the time of the survey. Third, this study examined socioeconomic inequalities in child vaccination at the national level. Since there may be different associations between factors at the subnational level in different countries, the generalisability of the findings should not be extended to population groups within the country. Finally, this study focused only on wealth-related inequalities in child vaccination coverage and did not examine other social inequalities in vaccination coverage (eg, race/ethnic-related inequalities) that may be present in the sampled countries.
Caveat considered, this study suggested that pro-rich distribution of child vaccination in most low/middle-income countries remains an important public health policy concern and policies aimed to improve ANC among mothers in lower socioeconomic groups may mitigate socioeconomic inequalities in vaccination coverage in low/middle-income countries.
What is already known on this subject
There have been several international initiatives set out to improve child immunisation rates in low/middle-income countries over the last four decades. These initiatives led to a significant increase in child vaccination coverage globally, which, in turn, reduced child mortality and morbidity due to infectious diseases in several countries. Despite the remarkable global improvement in child vaccination coverage, the improvement is not equally distributed among the countries. There is also a growing body of evidence suggesting socioeconomic inequalities in child vaccination within low/middle-income countries.
What this study adds
Although the current studies indicated socioeconomic gradients in child vaccination in low/middle-income countries, few studies have summarised the magnitude of socioeconomic inequalities across countries. There are even fewer studies that have examined the determinants of socioeconomic inequalities in child vaccination across countries. This study provides a comprehensive analysis of socioeconomic inequalities in vaccination coverage in 46 low/middle-income countries. The results suggested that pro-rich distribution of child vaccination in most low/middle-income countries remains an important public health policy concern. Policies aimed at improving antenatal care among mothers in lower socioeconomic groups may mitigate socioeconomic inequalities in child vaccination in low/middle-income countries.
Acknowledgments
MH gratefully acknowledges MEASURE DHS for their permission to use the Demographic Health Surveys (DHS) data. MH thanks two anonymous reviewers and the associate editor for their helpful comments and suggestions. MH also acknowledges the comments from participants in the Canadian Immunization Research Network and the Canadian Center for Vaccinology (CIRN/CCfV) Education Series at Dalhousie University.
References
Footnotes
Contributors MH is the single author of the paper.
Funding The author has not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval This study was not subject to ethical approval because it did not involve data concerned with human participants. The study used secondary data from Demographic Health Surveys (DHS, http://www.dhsprogram.com/). The DHS surveys are fully available upon request without restriction.
Provenance and peer review Not commissioned; externally peer reviewed.