Article Text

Abstract
Background Son-biased sex ratios at birth (M:F), an extreme manifestation of son preference, are predominately found in East and South Asia. Studies have examined sex ratios among first-generation migrants from these regions, but few have examined second-generation descendants. Our objective was to determine whether son-biased sex ratios persist among second-generation mothers with South Asian ethnicity in Ontario, Canada.
Methodology A surname algorithm identified a population-based cohort of mothers with South Asian ethnicity who gave birth in Ontario between 1993 and 2014 (n=59 659). Linking to official immigration data identified births to first-generation mothers (ie, immigrants). Births not to immigrants were designated as being to second-generation mothers (ie, born in Canada) (n=10 273). Sex ratios and 95% CI were stratified by the sex of previous live births and by whether it was preceded by ≥1 abortion for both first-generation and second-generation mothers.
Results Among mothers with two previous daughters and at least one prior abortion since the second birth, both second-generation mothers and first-generation mothers had elevated sex ratios at the third birth (2.80 (95% CI 1.36 to 5.76) and 2.46 (95% CI 1.93 to 3.12), respectively). However, among mothers with no prior abortion, second-generation mothers had a normal sex ratio, while first-generation mothers gave birth to 142 boys for every 100 girls (95% CI 125 to 162 boys for every 100 girls).
Conclusion Son preference persists among second-generation mothers of South Asian ethnicity. Culturally sensitive and community-driven gender equity interventions are needed.
- migration
- ethnicity
- public health
- social epidemiology
- perinatal epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Globally, gender-based health inequity is related to the status of both women and men in society. The ratio of the sexes at birth (normally 103–107 boys to 100 girls) is an explicit measure of a gender-based health inequity. Son-biased sex ratios at birth have been identified in several Asian countries,1 most notably in several provinces in China and northern states of India, but also in Vietnam and Pakistan. Son-biased sex ratios are not static, with declines noted in Southern Asia, specifically in Sri Lanka, Nepal, Maldives and Bangladesh.2 Societies with a strong preference for sons have a rigid kinship system that exhibits both patrilineality and patrilocality.3 Patrilineality refers to sons inheriting productive assets (typically property), while daughters may be given only movable assets which are tied to marriage, such as a dowry (ie, payment from a bride’s parents to the groom). Patrilocality refers to the phenomenon where a daughter ceases to be a member of her birth family on marriage, joining her husband’s family and residing with in-laws. Related to these phenomena is the notion that a son is his parent’s old-age security. In addition, these societies may dictate important roles for sons in religious rituals and traditions, and have a desire to preserve female ‘purity’ as a reflection of family honour.4
Given that son-biased sex ratios are predominately seen in Asia, several studies have examined whether son-biased sex ratios persist among migrants from Asia. These studies conducted in the USA,5 the UK,6 Norway,7 8 Sweden9 and Canada10–14 have highlighted immigrants from a number of Asian countries including China,5 9 Korea,5 9 12 Vietnam,10 Pakistan7 and India.5 7–14 All immigrant groups except those from Pakistan were found to have son-biased sex ratios, particularly when examined after one or two previous daughters, suggesting that sex selection is a likely mechanism. Research from Canada makes the link to sex-selective abortion more explicitly by the finding that among Indian immigrant mothers with two previous daughters, the sex ratio doubled when the third birth was preceded by ≥1 abortion.13 It is hypothesised that gender bias may weaken with time since immigration to Western countries because the receiving society may not exhibit gender bias as explicitly or in the same manner and also because the perceived necessity for sons (eg, old-age security) would presumably be weaker in a receiving country such as Canada. Son-biased sex ratios were not found among mothers who immigrated from China to Canada.13 However son-biased sex ratios were found among Indian immigrant mothers residing in both Canada11 and Sweden9 and were present after more than 10 years since arrival.
Substantial immigration from India to the UK began in the 1850s15 and to Canada in the 1890s with immigration from other South Asian countries in the 1960s.16 17 Given this history, it is also important to identify whether son-biased sex ratios persist in second and subsequent generations of South Asian descendants. The results of previous research have been mixed—showing a persistence10 and a decline18 among Asian descendants. Given the heterogeneous study populations and mixed evidence, the objective of this study was to determine if son-biased sex ratios persist among second-generation mothers of South Asian ancestry in Ontario, Canada. Ontario is Canada’s most populous province (14.2 million people—40% of Canada’s total population)19 and home to 62% of all Canadians with South Asian origins (total ~1 million).20 Given this large population of South Asians, Ontario is an ideal setting for this study. These results will help determine whether promotion of gender equity and community-driven interventions would benefit solely first-generation immigrants or also second-generation descendants.
Methods
Population-based administrative databases were linked at the Institute for Clinical Evaluative Sciences (ICES) in Toronto, Ontario to conduct this retrospective cohort study. An encrypted unique identifier issued to all individuals eligible for coverage under the Ontario Health Insurance Plan (OHIP) was used to link individuals across databases. OHIP provides publicly funded healthcare coverage at no cost to all Ontarians. We included birth records to mothers who delivered up to three consecutive singleton live births in Ontario hospitals between April 1993 and March 2014. Mothers who did not have all their births in Ontario were excluded, along with all their children.
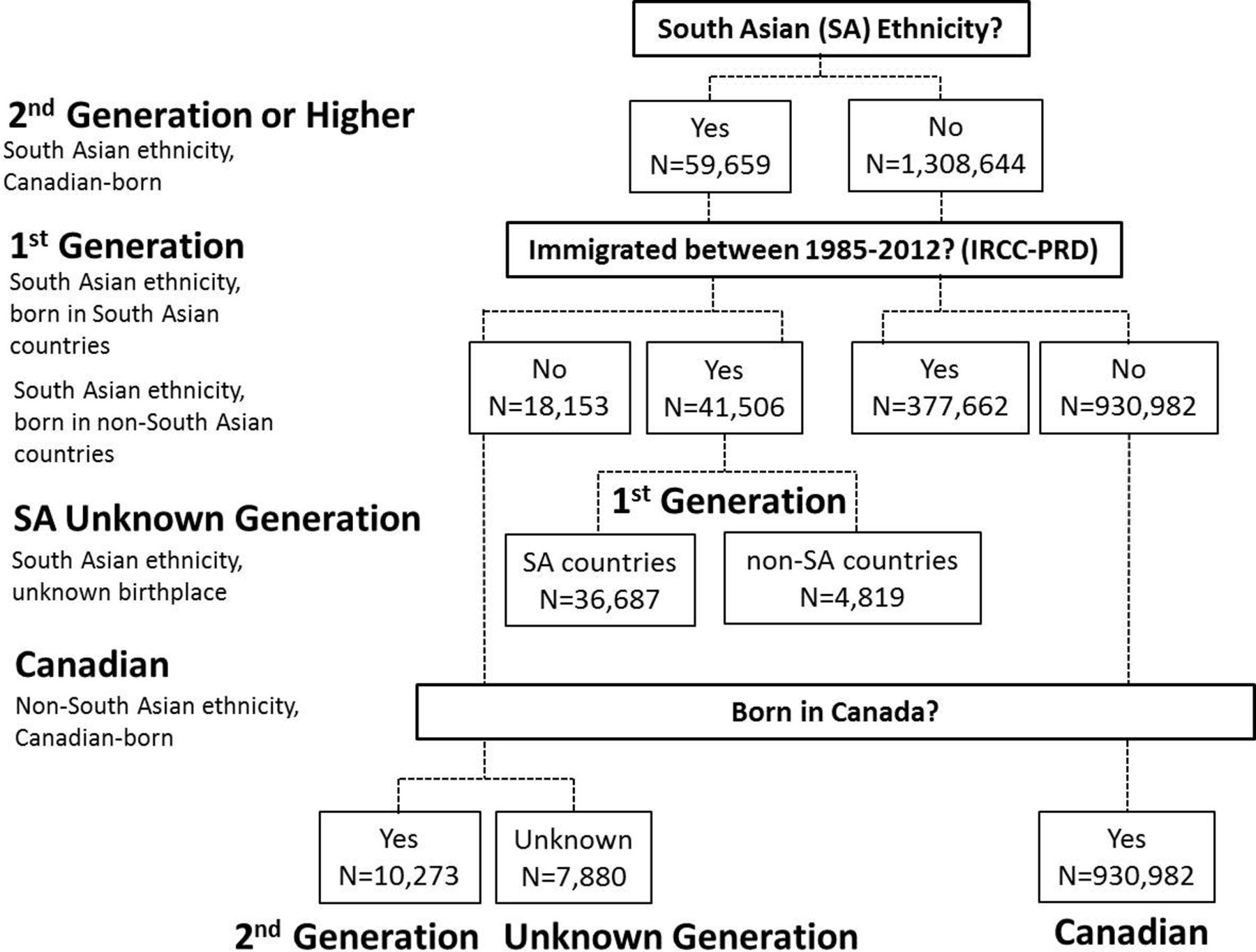
South Asian (SA) ethnicity was assessed using a surname algorithm developed at ICES,21 which classifies all mothers as being SA, Chinese or of unknown ethnicity. Specificity was high (99.7%); however, since surnames shared with other ethnicities were excluded, sensitivity was low (50.4%). Subsequent linkages of mothers with SA ethnicity to the Immigration, Refugee and Citizenship Canada Permanent Resident Database (IRCC-PRD) and OHIP database identified (1) second-generation mothers (born in Canada), (2) two groups of first-generation mothers (immigrated to Canada)—those born in SA countries and those born in non-SA countries—and (3) mothers of unknown generational status and unknown birthplace. These linkages are described in detail below.
Study groups
Two groups of immigrant mothers of SA ethnicity were identified by linking to the IRCC-PRD. The IRCC-PRD contains the legal immigration records of all individuals who obtained permanent residency in Canada from January 1985 to December 2012. The United Nations geographical classification system22 in conjunction with maternal country of birth reported in the IRCC database was used to classify immigrant women of SA ethnicity as being born in a SA country (figure 1—‘First-generation SA ethnicity, born in SA countries’) or a non-SA country (figure 1—‘First-generation SA ethnicity, born in non-SA countries’). About 90% of all individuals in the IRCC (88% for individuals from SA countries) were linked to a resident of Ontario with a valid health card number.23 Linked and unlinked individuals did not differ significantly by sociodemographic and immigration characteristics.
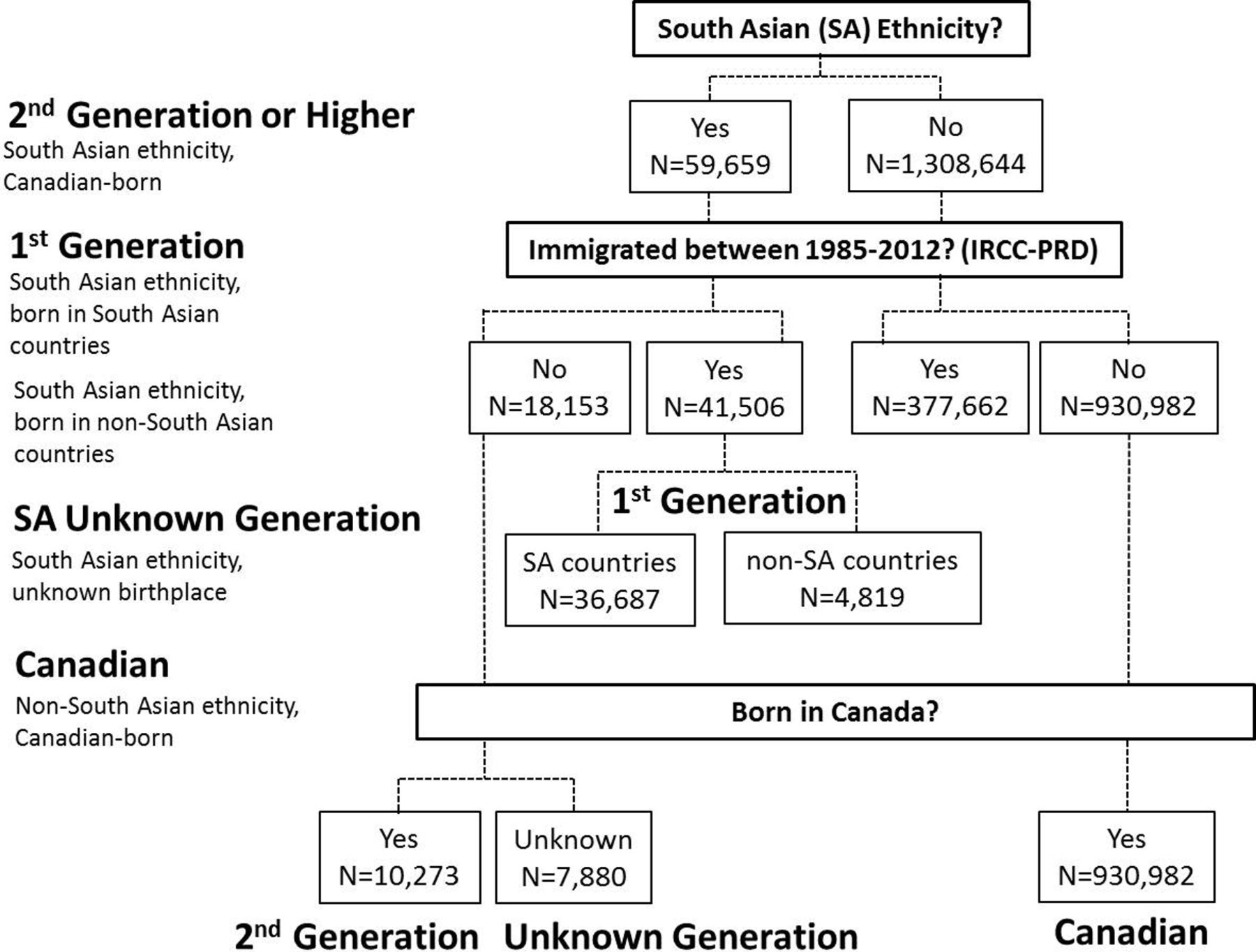
Identification of second-generation mothers of South-Asian ethnicity, first-generation mothers of South-Asian ethnicity and Canadian mothers. South Asian (SA) (United Nations Statistics Division 2013) countries include Afghanistan, Bangladesh, Bhutan, India, Nepal, Maldives, Pakistan and Sri Lanka. Non-SA countries include Guyana, Trinidad and Tobago, Kenya, Fiji and Tanzania, among others. IRCC-PRD, Immigration, Refugee and Citizenship Canada Permanent Resident Database.
Of the group of mothers not linked to the IRCC-PRD described above, linkage to the OHIP database identified mothers who became eligible for provincial universal health insurance in 1991 or after and had no record of being born in Ontario after 1988. These mothers are likely immigrants since immigration from South Asia increased steadily after 1991.24 This group of mothers consists of those who either (1) immigrated to Ontario between 1985 and 2012 but were not linked to the IRCC database (~12% of immigrants from South Asia), (2) immigrated to Ontario before 1991 or to Canada after 1991 and relocated to Ontario, or (3) were born elsewhere in Canada and relocated to Ontario. This group is designated as ‘SA Unknown Generation’ in figure 1.
Canadian-born mothers of SA ethnicity (figure 1—‘second generation’) primarily consisted of mothers of SA ethnicity that could not be linked to the IRCC database and had an OHIP eligibility start year of 1990. Ontarians with an eligibility year of 1990 includes those who became eligible in 1990 and those who became eligible before 1990, and therefore are more likely to be born in Canada since only 3.5% of Canada’s population were immigrants in 1991.24 Second-generation mothers also included those born in Ontario in or after 1988 or were born within 1 year of their OHIP eligibility date and therefore lived in Ontario for most of their lives.
Canadian mothers (figure 1—‘Canadian’) and all SA immigrant mothers (identified based on country of birth and not by the ethnicity database) were also examined.
Outcomes and covariates
Birth characteristics including infant sex and birth order were obtained from the Canadian Institute for Health Information’s (CIHI) Discharge Abstracts Database (DAD). Infant sex was defined as the biological sex at birth, male or female. Birth order was defined as the complete sequence of up to three consecutive live births from the same mother. We assumed that fertility decisions among second-generation and first-generation mothers of SA ethnicity were based on the number and sex of the children currently alive so at the time of each pregnancy the alive status of previous siblings was assessed via a linkage with the death database of the Ontario Office of the Registrar General and in-hospital deaths. If prior siblings were not alive by the estimated conception date of the current live birth, the birth order was revised accordingly for each subsequent live birth.
Mandatory reporting of induced abortions was captured in hospital acute care, day surgery and emergency department records from CIHI’s DAD, Same-Day-Surgery Database and the National Ambulatory Care Reporting System, respectively. These databases defined an induced abortion as any surgical or medically induced termination of pregnancy in the absence of a diagnosis of spontaneous abortion. Out-of-hospital abortions were captured using OHIP billing codes for a surgically induced abortion. If two abortion procedures were recorded within 40 days of each other for a given woman, they were considered the same event and the first abortion date was used. CIHI diagnosis codes and OHIP billing codes for induced abortion were described elsewhere.13
Analysis
Sex ratios, defined as the number of male newborns divided by the number of female newborns (M:F), were first stratified by the sex of previous live births. The overall sex ratio was estimated and further stratified by whether a woman had ≥1 abortion between the previous and index birth. Sex ratios were estimated for groups identified in figure 1 and for all immigrant mothers from SA countries. Intercept-only logistic regression was used to obtain 95% CIs around sex ratios.
For each group identified in figure 1, abortion rates (abortions per 100 women), relative to the period between the previous live birth and index child, were stratified by the sex of each child. Poisson regression was used to estimate rate ratios (RRs) and 95% CI comparing prior abortion rates when the index child was a boy compared with a girl for each strata of sex of the previous live birth.
Results
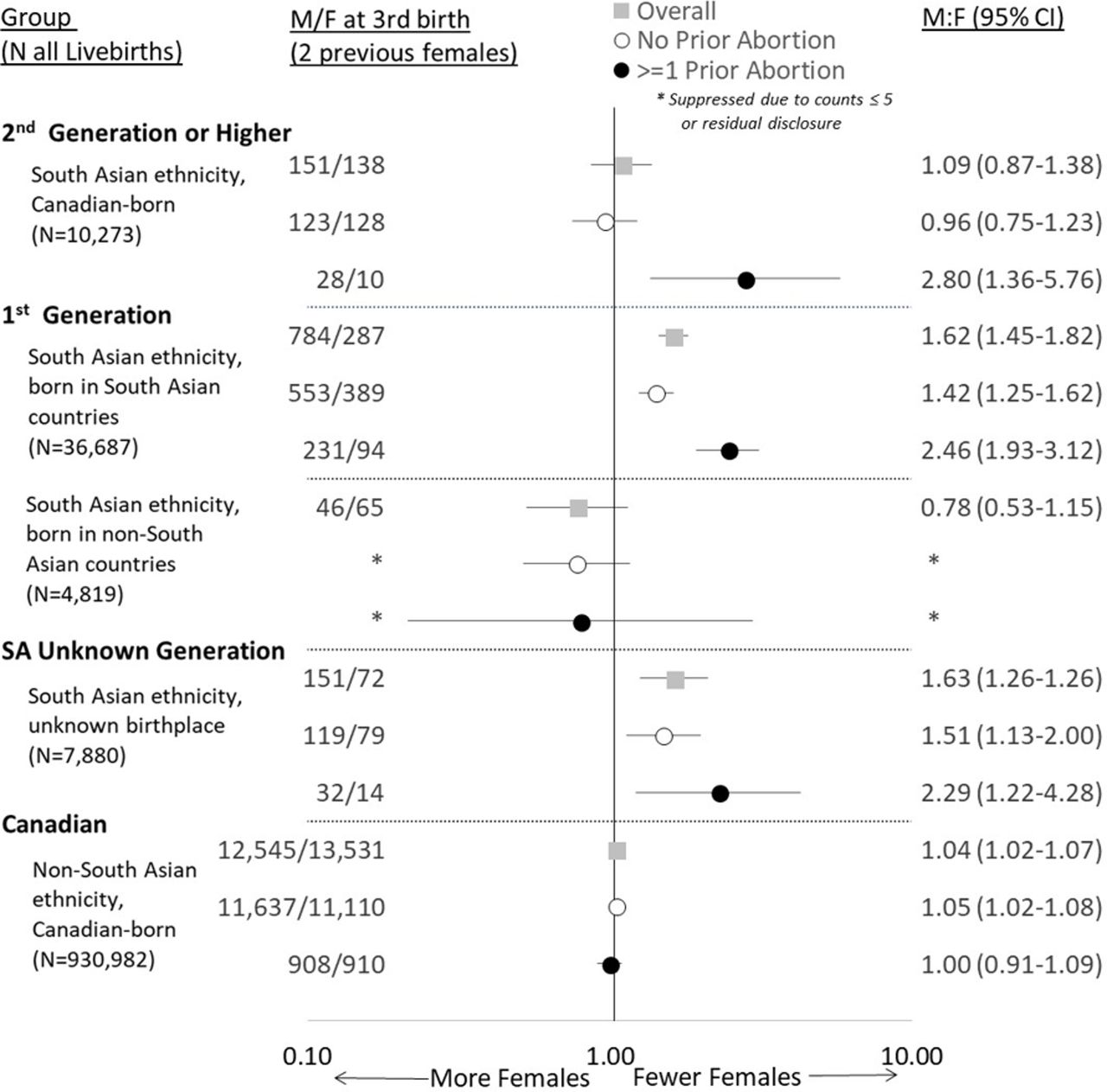
Figure 1 focuses on results from the third birth among mothers with two previous daughters since this is the only stratum for which M:F ratios were significantly elevated. Sex ratios at all birth orders are summarised in online supplementary table 1. The M:F ratio was significantly elevated among second-generation Canadian-born mothers with SA ethnicity with ≥1 prior abortion; 280 boys were born for every 100 girls (95% CI 136 to 576 boys for every 100 girls) but not among mothers with no prior abortions (see figure 2). Among first-generation mothers with SA ethnicity from SA countries with no previous abortions, 142 boys were born for every 100 girls (95% CI 125 to 162) while 246 boys were born for every 100 girls (95% CI 193 to 312) among mothers with ≥1 previous abortion. First-generation mothers with SA ethnicity with unknown birthplace had similarly elevated M:F ratios (1.51 (95% CI 1.13 to 2.00) and 2.29 (95% CI 1.22 to 4.28), respectively). We also note that there are approximately double the number of children born after two girls as opposed to after two boys for both first-generation mothers with SA ethnicity from SA countries and those with unknown birth place, also suggesting that the gender of children is an important consideration in family planning. Canadian mothers did not have elevated M:F ratios.
Supplementary file 1
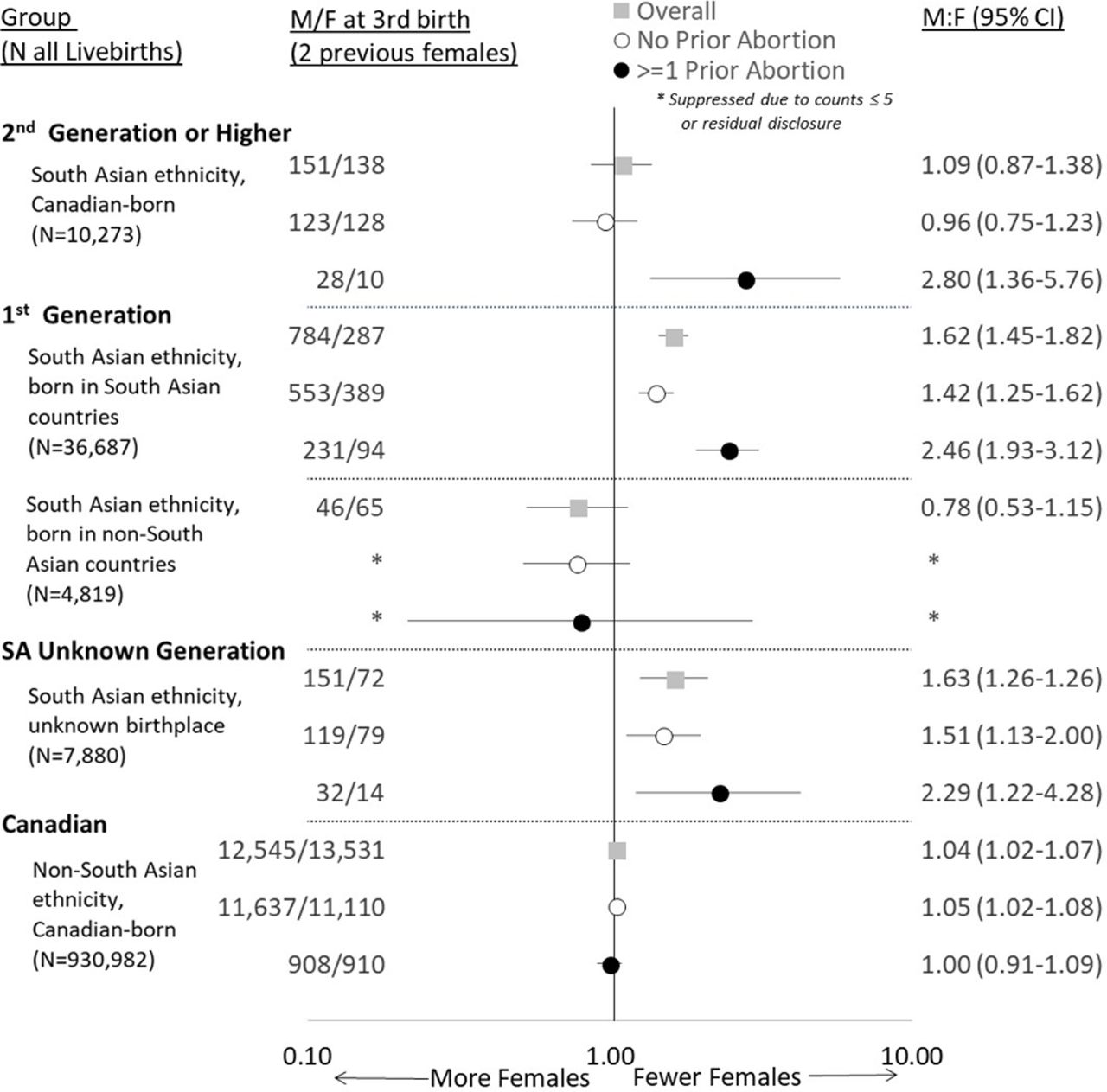
Male:female (M:F) ratios with 95% CIs at the third birth after two previous girls for second-generation and first-generation mothers of South Asian ethnicity and Canadian mothers. South Asian (SA) countries (United Nations Statistics Division 2013) include Afghanistan, Bangladesh, Bhutan, India, Nepal, Maldives, Pakistan and Sri Lanka. Non-SA countries include Guyana, Trinidad and Tobago, Kenya, Fiji and Tanzania, among others (listed in descending frequency).
In terms of abortion rates (table 1), across all strata of previous live births, second-generation Canadian-born mothers were less likely to have an abortion prior to an index birth compared with first-generation mothers with SA ethnicity from SA countries, except for prior to the first birth when it was three times higher among second-generation mothers. After having two girls, second-generation Canadian-born mothers with SA ethnicity were two times more likely to have an abortion prior to a third male child compared with a female child (RR 2.40, 95% CI 1.35 to 4.27). After two previous girls, two previous boys and one boy and one girl, first-generation mothers with SA ethnicity from SA countries were more likely to have an abortion prior to a subsequent male child compared with a female child (RR 1.75, 95% CI 1.44 to 2.14; RR 1.55, 95% CI 1.12 to 2.13; RR 1.28, 95% CI 1.04 to 1.57, respectively). Abortion rates prior to an index male child compared with a female child were not elevated for Canadian-born mothers.
Rate ratios (RRs) and 95% CIs for prior abortion comparing the sex of the index child, stratified by the sex of the preceding live birth for second-generation and first-generation mothers of South Asian ethnicity and Canadian-born mothers
Among all immigrant mothers from SA countries (n=98 816), M:F ratios were elevated for those with no previous abortion and for those with ≥1 previous abortion (1.23 (95% CI 1.14 to 1.32) and 2.12 (95% CI 1.75 to 2.51), respectively) (see figure 3). Of all immigrants from SA countries, only Indian mothers had elevated M:F ratios (1.64 (95% CI 1.46 to 1.84) and 3.30 (95% CI 2.62 to 4.16)). When immigrant mothers from India were excluded from South Asia, M:F ratios became non-significant.

{kind=link}
{kind=link}
{kind=link}
Male:female (M:F) ratios with 95% CIs at the third birth after two previous girls for immigrant mothers born in South Asia (N=98 517). South Asia (United Nations Statistics Division 2013) includes Afghanistan, Bangladesh, Bhutan, India, Nepal, Maldives, Pakistan and Sri Lanka. South Asian countries not included in figure had small sample sizes.
Discussion
Our study found important similarities and differences in the M:F ratios at the third birth comparing first-generation and second-generation SA women with two previous girls. First, both second-generation SA mothers and first-generation SA mothers from SA countries with ≥1 prior abortion between the second and third birth had almost three boys for every girl at the third birth. While the proportion of births occurring after ≥1 prior abortion between the second and third birth was lower among second-generation mothers (13%) compared with first-generation mothers (26%), it appears likely that some mothers in both groups selectively aborted at least one girl, which led to the excess in sons. Our analyses also indicated elevated abortion rates after two previous girls and prior to having a male child compared with a female child for both second-generation and first-generation mothers, providing further support for sex-selective abortion.
In contrast, second-generation mothers of SA ethnicity with no prior abortion between the second and third birth did not have an elevated M:F ratio, while it was elevated for first-generation mothers of SA ethnicity born in SA countries. The elevated M:F ratio among first-generation mothers suggests that, despite there being no prior abortion recorded in Ontario, some women may have sought abortion outside of Ontario or used sex-selective technology outside of Canada (since it is prohibited in Canada25). The normal M:F ratio among second-generation mothers of SA ethnicity with no prior abortion suggests that mothers in this group are less likely to use alternative paths to sex selection compared with their first-generation counterparts. The overall proportion of births that occurred after ≥1 abortion was higher among second-generation mothers than first-generation mothers (17% vs 12%), so it may be that second-generation women were better acquainted or comfortable with the Ontario healthcare system. An alternative interpretation is that the importance of sons has diminished since a subgroup of second-generation mothers is not engaging in sex-selective abortion in Ontario or abroad.
These analyses also show son-biased sex ratios are absent among immigrant mothers born in SA countries other than India, despite the fact that many SA countries, not just India, have had or still have son-biased sex ratios.2 There may be two explanations for this. First, numerous arrival cohorts were aggregated in these analyses and could be obscuring son-biased sex ratios in specific arrival cohorts. Second, the number of immigrants from other South Asian countries is about half that of India, making it difficult to detect son bias. This suggests there is a remote possibility that second-generation descendants of non-Indian ancestry contributed to the son-biased sex ratio.
The only two studies that could be identified which examined son-biased sex ratios in second-generation South Asians used Canadian data. One study reported that the M:F ratios at the third birth after two previous girls was 1.50 for the first generation of South and East Asians and 1.32 for second generation, indicating son-biased M:F ratios were present in both generations but diminished in the second.10 While these findings are generally consistent with the current study, our findings are more specifically focused on South Asians and point more clearly to the mechanism driving son-biased sex ratios by stratifying by prior abortions. A report suggested that second-generation or subsequent-generation East Indians were less likely to prefer sons since they had a lower proportion of male live births (50.8%) than first-generation East Indians (52.7%); however, these results were not stratified by the sex of previous births or prior abortion.18
Our finding of persistent son-biased sex ratios among second-generation SA women is a surprising one, given the emphasis first-generation South Asian immigrant parents place on educating their second-generation daughters.16 26 However, it seems that the promotion of higher education among second-generation daughters has little to do with contributing to the responsibilities that are typically reserved for sons (ie, supporting parents). A qualitative study suggests that the purpose of promoting education among second-generation daughters was to uphold the image of a ‘model minority’ (ie, hard-working, disciplined and successful), restrict social engagements outside the home (ie, limit western influence) and improve marriageability.26 Importantly, if second-generation daughters continue to adhere to patrilocality (ie, residing with in-laws after marriage), it is difficult, and perhaps impossible, for parents to benefit from their daughter’s higher education and income. Studies in India have shown that higher maternal education is either not associated with son-biased sex ratios27 or that it is associated with greater knowledge of and access to sex-selective technology.28 This situation among second-generation mothers certainly exemplifies a ‘double burden’ where women are educated and work outside the home but are also expected to maintain their traditional roles within the family. In the immigration context, however, interpersonal and structural discrimination faced by SA families in Canada may negatively affect the ability to dismantle deeply entrenched and harmful gender norms.16 29
Our study has strengths and limitations. Two important strengths of this work are the strong ability of the surname-based algorithm to exclude those who were not truly of SA ethnicity, as well as the high linkage rate of the immigration database to the healthcare database. An important limitation is that we are not certain that all second-generation mothers with SA ethnicity were born in Ontario. Since the majority of second-generation mothers were identified based on an OHIP eligibility start year of 1990, immigrants may have been inadvertently included. We estimate that ~10% of all second-generation mothers of SA ethnicity may be immigrants. Given this small proportion and that misclassified immigrants would not be differentially concentrated only among those with ≥1 previous abortion, it is unlikely that the son-biased sex ratios identified can be attributed to misclassified immigrants. Another limitation of the SA surname algorithm is the poor ability of the algorithm to identify all those who are truly of SA ethnicity. However, those with SA ethnicity not identified by the algorithm have been excluded (figure 1, right side—two groups with n=377 662 and n=933 982) and do not influence our interpretation of second-generation and first-generation mothers. We could not capture abortions done outside of Ontario or the use of sex-selective technology outside of Canada; however, strong effects were found among those with at least one prior abortion despite this limitation biassing the results towards the null, which leaves our interpretation unchanged. Finally, we identified a severe form of female discrimination among a subset of second-generation and first-generation South Asian mothers, but more subtle forms of gender bias may be more pervasive.
Conclusion
We do not know why some first-generation and second-generation mothers with SA ethnicity opted to have an abortion. All women in Canada have the legal right to choose abortion without having to provide their reasons for doing so.30 However, South Asian community agencies suggest that women may not view abortion as exercising personal choice but as a necessity given intense familial and cultural pressures to have a son.31 A Canadian qualitative study describes son preference in the Punjabi immigrant community as result of intersecting power dynamics (ie, age, gender, patriarchy, transnational family ties), which allows older immigrants in the community to perpetuate the importance of sons over daughters.29 The impact of these dynamics on mothers range from internalised patriarchy32 to explicit coercion33 and may result in some women seeking sex-selective abortion or using sex-selective technology. Suggestions to criminalise sex selection, force disclosure for the reasons for abortion34 or prevent families from finding out the sex of their child35 36 reinforces interpersonal and structural discrimination against SA women and may encourage women to seek these services elsewhere or access unsafe abortions endangering women’s lives. Instead, we suggest an important next step is to understand how reproductive decision-making occurs in Indian families and other SA groups and whether this can be re-negotiated to promote gender equity in a culturally appropriate way, which places greater value on the well-being of both mothers and daughters. Our study suggests that such community-based interventions would benefit both first-generation women and second-generation women of SA ancestry, particularly those originating from India.
What is already known on this subject
Son-biased sex ratios at birth (in excess of the normal ratio—103 to 107 boys for every 100 girls) have been found in some East and South Asian countries. Some studies have identified son-biased sex ratios among first-generation immigrants from these countries; however, few studies have examined second-generation descendants despite large diasporas in many immigrant-receiving countries.
What this study adds
Our study finds that son-biased sex ratios at birth persist among second-generation mothers specifically of South Asian ethnicity in Ontario, Canada, which were associated with prior abortion. Among first-generation mothers born in South Asian countries, only those from India had son-biased sex ratios suggesting that second-generation mothers with son-biased sex ratios likely have Indian ancestry.
Acknowledgments
This study was supported by the Institute for Clinical Evaluative Sciences, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. The authors would like to thank Baldev Mutta (Punjabi Community Health Services in Brampton, Ontario, Canada) as well as Kripa Sekhar (South Asian Women’s Centre in Toronto, Ontario, Canada) for their input on this study.
References
Footnotes
Contributors SW and MLU conceived the research question and designed the study. SW conducted statistical analysis, interpreted the results and wrote the first and subsequent drafts of the manuscript. PU, MB, AJ and DS contributed to data interpretation and revisions of the manuscript. MLU obtained funding. All authors approved the final version of the submitted manuscript.
Funding This study was funded by a grant from the Canadian Institutes of Health Research (CIHR). SW’s postdoctoral fellowship is supported by a grant from CIHR. MLU holds a Canada Research Chair in Applied Population Health from CIHR.
Disclaimer The opinions, results and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by the Institute for Clinical Evaluative Sciences or the Ontario Ministry of Long-Term Care is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute of Health Information. However, the analyses, conclusions, opinions and statements expressed herein are those of the authors and not necessarily those of the Canadian Institute for Health Information. PU was employed at the Ontario Non-Profit Network (ONN) at the time this paper was written; however, her contribution to this paper is not related to her role at the ONN and therefore the results, conclusions and opinions expressed are not those of the ONN.
Patient consent Not required.
Ethics approval This study was approved by the institutional review board at Sunnybrook Health Sciences Centre and the Research Ethics Board at St. Michael’s Hospital, Toronto, Canada.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from this study available.