Article Text

Abstract
Background Homelessness is associated with increased mortality, and some predictors of mortality have been previously identified. We examined the overall and cause-specific mortality among homeless men in Helsinki and the associations of social background and health service use with mortality.
Methods To assess cause-specific mortality in a competing risks framework, we performed a register-based, case–control study of 617 homeless men and an age-matched control group of 1240 men from the general population that were followed for 10 years between 2004 and 2014. Cox proportional hazards model was used to calculate HR for death and a competing risks model to calculate sub-HRs (sHR) for cause-specific death.
Results During the follow-up, 45.0% of the homeless died compared with 10.5% of controls (HR 5.38, 95% CI 4.39 to 6.59). The risk of death was particularly elevated for the homeless aged ≤50 years (HR 10.3, 95% CI 7.0 to 15.2). External causes caused 34% of the deaths (sHR 11.2, 95% CI 6.8 to 18.2), but also deaths from medical causes were common (sHR 3.6, 95% CI 2.9 to 4.6). Age and somatic hospitalisation were significant predictors of death both among homeless and controls. Educational attainment, marital status, employment and psychiatric hospitalisation were significant predictors of mortality among the controls, but not among the homeless.
Conclusions Homelessness is associated with a fivefold mortality compared with the controls, and especially homeless aged ≤50 years have an increased risk of death. Being homeless eliminates the protective effects of marriage, employment and education on mortality risk.
- homelessness
- mortality
- cohort studies
- substance abuse
- accidents
Statistics from Altmetric.com
Introduction
Not having a home impedes your possibilities to care for your health and well-being. Hence, homelessness is associated with increased morbidity and mortality.1 Studies have reported standardised mortality ratios (SMRs) between 2.0 and 5.6 among the homeless compared with the general population.1–10 This excess mortality is higher within younger age groups and decreases with age.2 5 8 11 12
Among the homeless, elevated risks of death have been reported for medical conditions, including infections,4 5 diseases of the digestive system4 5 11 12 and blood-forming organs,4 5 neoplasms4 5 11 and for respiratory,4 5 12 psychiatric4 5 cardiovascular4 5 11 and cerebrovascular12 diseases. Further, external causes, such as poisonings, suicides, homicides and accidents, are responsible for many deaths in homeless cohorts.2–5 11–13
Being single and having short education are known predictors of mortality in the general population.14 15 Their associations with mortality have not previously been studied among homeless. Unemployment is also a known predictor of mortality in the general population.16 A Danish study3 showed that having income from employment decreased the risk of death also among homeless. Other previously identified predictors of mortality among homeless are substance use disorders (SUDs),2–4 6 17 18 non-immigrant background,3 4 white race,8 11 previous incarceration6 and extended homelessness.6 7 French and US studies found that deaths were more common during winter season19 20; however, this association was not observed in the Canadian study.21 Contrary to findings from the general population where psychiatric morbidity is a known risk factor for premature death,22 there is evidence that homeless persons with psychiatric illness other than SUDs have a lower mortality compared with the homeless on average.2 3 6 7 18 Danish studies have shown that having more than 10 contacts with shelters during first year of contact increases mortality,3 as does having short and repeated stays in shelters within a year.2
Previous studies on causes of deaths among homeless have relied on comparisons with the general population producing SMRs and relative risks (RRs). However, comparing with standardisations from the general population within age bands increases the margin of error compared with case–control set-ups, and particularly in populations with high mortality, accounting for competing risks also becomes relevant.23 24 Using a matched control group from the general population, we were able to estimate the all-cause HR and the cause-specific sub-HRs (sHRs) for death in the presence of competing risks. The aims of the study were to examine the overall and cause-specific mortality among homeless men and to assess the associations of educational attainment, marital status, employment and healthcare use with the overall mortality risk among the homeless and among their controls.
Methods
Study population
The study population consists of all homeless men that stayed in Herttoniemi shelter for men in Helsinki during 2004 (n=624). Herttoniemi shelter was the only homeless shelter in Helsinki operating on a walk-in basis at that time. The other temporary accommodations provided for homeless were more permanent placements that required promissory notes from a social worker. Thus, our sample is a total sample of male shelter users in the City of Helsinki in 2004. Herttoniemi shelter could accommodate 75 men each night. The shelter was free of charge and without sobriety requirements for all homeless men residing in Helsinki. Clients had to report their personal identification codes when registering for the night, and thus, shelter services were not available for the migrant and undocumented population. In 2004, homeless women were accommodated in a separate shelter, the register of which we did not have access to, and therefore women are excluded from this study. Study entry was assumed to be 1 July 2004. Risk time was calculated from the number of days between study entry and date of death, emigration or end of follow-up (31 December 2014), whichever came first. A control group was obtained from an age-matched random sample of men from the Population Register Center, matching criteria being residing in the same municipality and being born within the same month in a 2:1 ratio (n=1248). Three persons in the control group were also cases in the homeless sample and were thus excluded. Further, those who emigrated or deceased before the start of follow-up 1 August 2004 (n=7 in the homeless sample and n=5 in the control group) were excluded, producing a cohort of 617 homeless and 1240 controls.
Registers used
The social service client register at the City of Helsinki was used to identify persons attending the shelter in 2004 and their number of shelter nights that year. The registers of Statistics Finland were used for retrieving information on socioeconomic status, education and time and cause of death. The Finnish Cause of Death Register records data on the deaths. The diagnoses of the causes of death are made by regional medical officers and physicians, and registered in the Finnish Cause of Death Register kept by statistics Finland. The quality of the register has been found to be good.25 The National Care Register for Health Care includes data on all hospital inpatient episodes on an individual level. We used the register to get data on health service use and diagnosis. Information on marital status was obtained from the Population Register Centre. Personal identification codes, which are unique for all Finnish citizens and permanent residents, were used to link the information.
Mortality, causes of death and predictors of interest
The cause of death was determined by the underlying cause of death [International Classification of Diseases, 10th Revision (ICD-10)] in the Cause of Death Register, which also provided the time of death. We analysed separately deaths from diseases and medical causes (divided into cardiovascular diseases, neoplasms, diseases of the digestive system, diseases of the respiratory system and other diseases and medical causes) and deaths from external causes (divided into accidental poisonings and other external deaths).
We examined the associations of the following sociodemographic factors at baseline: age (continuous variable), education (higher than the 9 years basic level or not), employment (employed or not) and marital status (married/registered partnership or not) with mortality. We also controlled for healthcare contacts 6 months prior to baseline (1 January–30 June 2004) to examine the effect of previous care contacts on the association between homelessness and mortality. The healthcare contacts examined were emergency room visits, outpatient visits at specialist care level and hospitalisations. Since psychiatric morbidity (other than SUDs) has been shown to be associated with lower mortality2 3 6 7 18 and SUDs with higher mortality2–4 6 17 18 among homeless, we analysed separately the associations between death and hospitalisations due to (1) psychiatric diagnoses excluding SUDs (ICD-10: F00–F09, F20–F99) and (2) SUDs (F10–F19). Because death due to external causes is more common among homeless,2–5 11–13 we also separately analysed associations between death and hospitalisations due to (3) traumas and injuries (S00–T99) and (4) other somatic diagnoses to see if prior hospitalisation for traumas predicts death among homeless. All predictors apart from age were used as dichotomous factors in the multivariate Cox model (ie, contacts vs no contact for the healthcare variables).
Statistical analysis
Study entry was chosen to be 1 July 2004 (ie, halfway into year 2004). Risk time was calculated from the number of days between study entry and date of death, emigration or end of follow-up (31 December 2014), whichever came first. Time-to-event analysis was based on the Kaplan-Meier failure function. Cumulative mortality is also shown using age as the time scale. We used Cox proportional hazards model to calculate the overall HR for death and the Fine and Gray competing risks proportional hazards model26 to calculate the crude and age-adjusted sHR for different causes of death. Using a multivariate Cox proportional hazards model, we estimated the effects of our predictors on the HR; this analysis was done separately for the control group and for the homeless population. The results are presented as HR and sHR with 95% CIs. The proportional hazards assumption was tested graphically and by use of a statistical test based on the distribution of Schoenfeld residuals (the assumptions were successfully fulfilled). Statistical comparisons were made by using the t-test and the χ2 test. As the data for health service use were highly skewed, bias-corrected and accelerated bootstrap estimation (5000 replications) was used to derive 95% CIs, and differences between the means were tested by bootstrap-type t-test. All analyses were performed using STATA 14.0.
Results
The mean age of the homeless at time of sampling was 48.7 years (range 21–78 years) (table 1). Mean accumulative stay in shelter was 28.7 nights, but over half (52.7%) of the homeless had stayed less than four nights in the shelter during 2004 (data not shown). In the study population, few were married or living in a registered partnership (5.3%) compared with the control group, where a majority (52.3%) were married or living in a registered partnership. Only 5.3% of the homeless were employed during the year 2004 compared with 66.5% of the controls (p<0.001).
Baseline characteristics of homeless in Helsinki and control group (N=1857) year 2004
The healthcare use prior to baseline differed significantly between the homeless and the control group: 32.2% of the homeless had been hospitalised during the 6 months prior to baseline compared with 4.7% of the control group (p<0.001). Similarly, 36.3% of the homeless had emergency department visits compared with 5.6% of the control group (p<0.001). The homeless population and the control group had the same average number of outpatient visits to specialised care (on average 0.4 visits during the 6 months examined), but a larger proportion of the homeless had outpatient visits than the control group (homeless 19.9%, controls 13.1%, p<0.001).
Mortality and causes of death
By the end of the 10-year follow-up, 287 homeless men (46.5%) and 138 controls (11.1%) died, giving a hazard rate of 5.38 (95% CI 4.39 to 6.59) for all-cause mortality. Among those who had died during the follow-up, the mean age of death was 56.5 years among the homeless compared with 63.7 years among the control group. The deaths were evenly distributed over the year in both groups (data not shown).
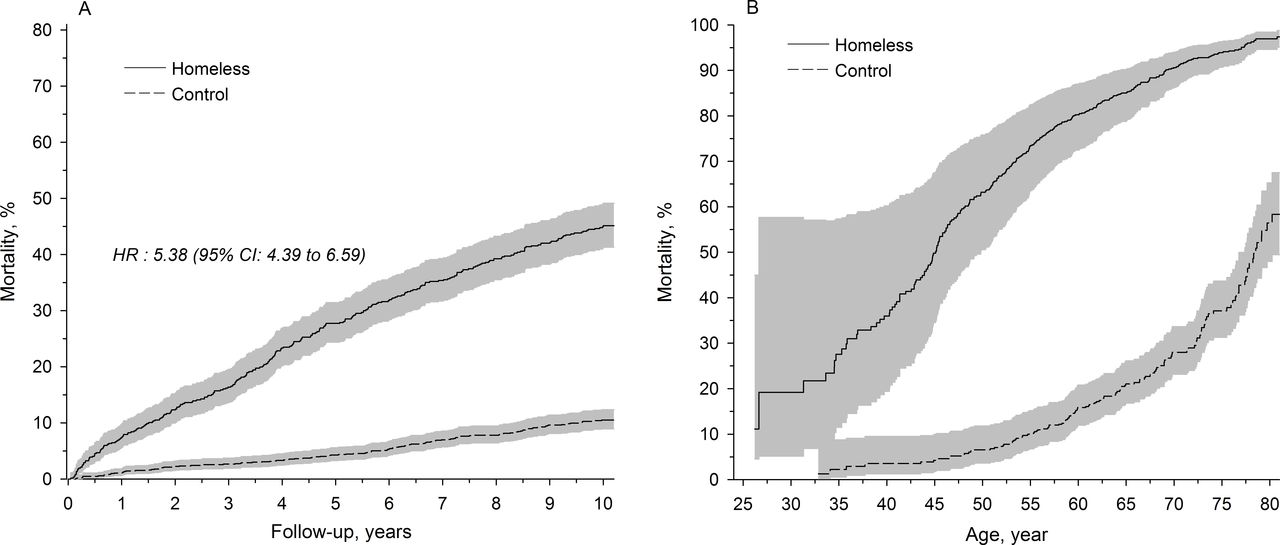
After the first 5 years of follow-up, the difference in mortality rate of the homeless compared with the control group was even higher than that at the end of follow-up (27.7%, 95% CI 24.5 to 31.4; 4.3%, 95% CI 3.3 to 5.6, respectively; figure 1A). Mortality rates were particularly high among the younger homeless, as demonstrated in figure 1B. By the end of the follow-up, 38.0% of the homeless who were under 50 years old at baseline had died, whereas death was rare (4.7%) in the control group of the same age. The HR for death for the homeless under 50 years at baseline was 9.83 (95% CI 6.44 to 14.76; figure 2).

Ten-year follow-up of the mortality of homeless men in Helsinki between 2004 and 2014. The mortality rate of the homeless (n=617) and control group (n=1240) by time (A) and by age (B).
{kind=link}
{kind=link}
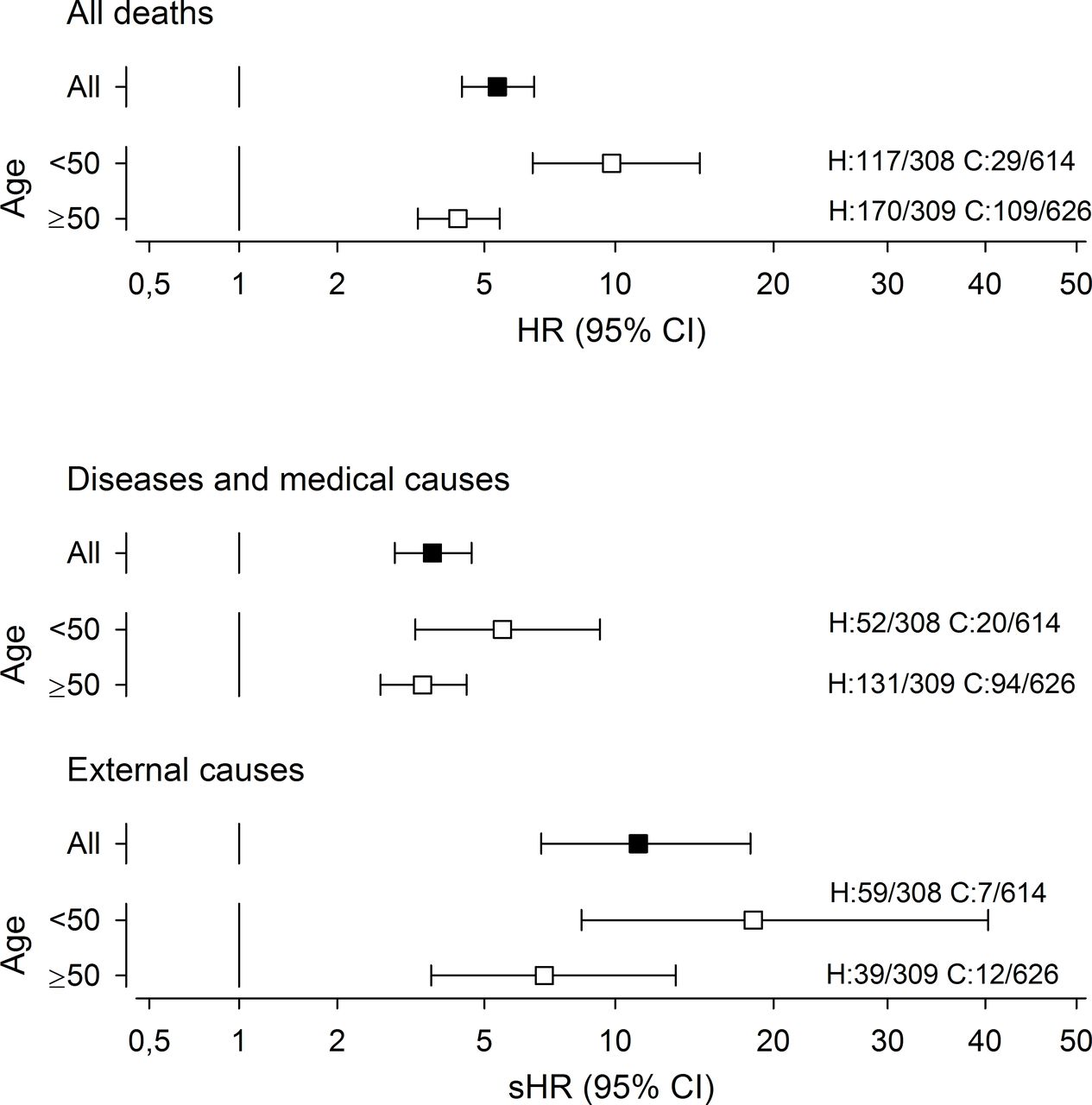
All-cause mortality and mortality by medical causes and external causes, respectively, for 617 homeless (H) men compared with 1240 controls (C), HRs and sub-HRs (sHR) with 95% CIs, total sample and presented by age group. The ratios of deaths per cases for each group are shown at the right-hand side of the figure.
Deaths by external causes were responsible for 34.1% of all homeless deaths (n=98) (table 2). Half of the deaths from external causes were due to poisoning (sHR 25.45, 95% CI 9.19 to 70.45). The risk of death due to medical causes was also high with an sHR of 8.22 (95% CI 4.11 to 16.43) for diseases in the digestive system (including alcohol induced cirrhosis) and 3.37 (95% CI 1.47 to 7.49) for respiratory diseases. The sHR for death from external causes was 11.18 (95% CI 6.85 to 18.25), as shown in figure 2, and was particularly high among the homeless under 50 years of age at baseline.
Causes of death and sHR among homeless men in Helsinki 2004–2014 calculated using an age-adjusted Fine and Gray hazards model (N=1857)
Effects of sociodemographic factors and health service use on mortality
We performed multivariate Cox regression analyses to assess the effects of age, educational attainment, marital status, employment and health service use on mortality separately among the homeless and control group (table 3). For the control group age (HR 1.06, 95% CI 1.04 to 1.08), not being in employment (HR 2.36, 95% CI 1.54 to 3.62), not being married/in a registered partnership (HR 1.85, 95% CI 1.30 to 2.63) and having only basic education (HR 1.84, 95% CI 1.30 to 2.61) increased the risk of death significantly. The same factors did not predict death in the homeless population. Outpatient visits, emergency department visits and hospitalisations for trauma did not predict death in either group. Psychiatric hospitalisation 6 months prior to baseline was a risk factor for death among the control group (HR 2.90, 95% CI 1.11 to 7.58) but had no effect among the homeless (HR 0.92, 95% CI 0.65 to 1.29). The only significant predictors of mortality among homeless were age (HR 1.03, 95% CI 1.02 to 1.04) and hospitalisation due to somatic conditions (HR 1.48, 95% CI 1.07 to 2.04), but the effect was stronger for both these factors in the control group (HR 1.06, 95% CI 1.04 to 1.08 and 2.86, 95% CI 1.44 to 5.68, respectively). Having less than four shelter nights during 2004 did not predict death among homeless (HR 1.15, 95% CI 0.90 to 1.45) and was not included in the final model (data not shown).
Predictors of death among homeless men in Helsinki (n=617) and the control group (n=1240), multivariable Cox proportional hazards model
Discussion
We examined all-cause and cause-specific mortality during a 10.5-year follow-up and the effects of several potential predictors of death among homeless and the general population and found that the overall risk for death among homeless shelter users in Helsinki was high (HR 5.38, 95% CI 4.39 to 6.59) compared with previous studies.1 2 4–10 Only Nielsen et al reported a higher figure for Danish shelter users.3 Our study was the first case–control study on causes of death among homeless and clearly demonstrates what previous studies2 5 8 11 12 have suggested that the excess mortality is particularly high in younger age groups and then decreases with age. The risk of death was significantly increased for the homeless in all selected groups of diseases and medical causes. The highest risk of death was in the group of diseases of the digestive system, where alcoholic liver disease formed the largest group being responsible for 36 of the 40 deaths in the homeless cohort. The risk of death by external causes was even larger than that for diseases and medical causes being over 11-fold compared with the control group. This was particularly true for homeless under 50 years of age. Compared with previous studies,4 5 Finnish homeless men have a high risk of death for external causes. Only Nielsen et al 3 reported mortality rates for death from unintentional injuries higher than ours among homeless in Denmark. However, due to differing classifications of external causes of death, direct comparisons of figures could not be done. Looking at the deaths by external causes in our study, we see that SUDs are responsible for many deaths with accidental poisoning having an sHR of 25.45. Overall, we conclude that deaths related to SUDs were overrepresented among the homeless, supporting the findings of Beijer et al 4 that the excess mortality among homeless is related to alcohol and drug abuse. Our data included relatively few suicides (n=7), contradicting previous studies that have found suggestive evidence of suicide risks increasing among the homeless population.1 Because of small numbers, we calculated no sHR for suicides, but looking at total numbers alone, we had a less than twofold RR compared with Danish studies with a RRs for suicides between 6.0 and 7.3.2 ,3 A Canadian study reported suicide risks of 2.3–3.3.5 On the other hand, homicides were relatively prevalent (n=7) in our cohort. We had an equal number of deaths by suicides and homicides, whereas the relationship in the control group was 8:1, similar to that of the relationship seen in the whole country.27
Comparing our mortality rate and results from previous studies,2–8 10 a pattern can be seen with higher excess death rates among homeless in Scandinavia and Scotland than in North America. It is possible that in societies with advanced social protection systems, homelessness due to poverty and unemployment alone is more often prevented. Thus, the shelter population in these settings may be characterised by greater morbidity and social problems than in countries with less intensive social protection systems. This may in itself increase the risk for death and explain the higher mortality rates in Northern European study populations compared with populations from North America. The substantial differences in healthcare use present already prior to baseline in the homeless cohort compared with the control group indicate that the homeless suffered from increased morbidity already at baseline, probably contributing to the high mortality. The mortality rate in our cohort was especially high considering that our population, like Finnish shelter population typically,28 was older than most previously studied populations and that excess mortality of homeless people has been shown to decrease with age.
Contrary to findings from France and the USA,19 20 we saw no increase in deaths during winter months despite the cold climate in Finland. This is in line with findings in the Canadian study.12 There were only two deaths due to hypothermia among the homeless in our study (data not shown). This relative absence of deaths due to hypothermia could be a result of Finnish legislation obliging the municipalities to provide all residents with shelter.
We found that increased age and somatic hospitalisations predicts mortality among homeless, and even more so in the control population. In accordance with many previous studies14–16 also employment, marriage and education decreased the risk of mortality in the control group. However, these predictors had no relevance in predicting death among the homeless in our study. As in the Danish study3 where being employed decreased the risk of death also among homeless, we did see a small effect of not being employed on mortality risk, although statistically insignificant, possibly due to the few employed persons in our cohort. These results further support the theory that in a system with relatively well-developed welfare services, those who must rely on shelter services are marginalised to a point where the effect of this marginalisation over-rides the protective effects of educational attainment, marriage and employment.
We did not see an increase in mortality with increased total number of shelter nights. Previous findings have shown that many and short contacts with shelters increase the mortality risk, indicating that the transient homeless population is most at risk.2 3 Our findings neither support nor contradict this theory but add to the knowledge of the relationship between the number of shelter nights and mortality by showing that already very few nights in shelter pose an increased risk of death.
Our study has several strengths and limitations. By using a matched control group from the general population and a competing risk proportional hazards model, we were able to produce cause-specific sHRs for causes of deaths for the first time. There is only one previous case–control study on mortality of homeless,10 but it had a shorter follow-up (5 years) than our study and did not report causes of death. By matching the controls locally to place of residence, we also reduced the risks of local effects in the cause-of-death coding practices. However, there are probably many more potential confounding factors that might explain the increased risk of death such as undiagnosed disorders, lifestyle factors, family background and traumas in childhood, lack of social networks and capacity to handle crisis. We were unable to adjust for these factors in our study as they are not recorded in the registers. The long follow-up time produces new knowledge on how the mortality risk develops over time, but the time lag between exposure and outcome possibly also lessens the effects of our predictors on mortality. It would have been interesting to study time-dependent variables and their association to the mortality risk, but unfortunately, we had no access to such data. Another limitation of the study is the short follow-up period of healthcare service use prior to baseline (6 months); as a measurement of the morbidity in the cohort, a longer period would have given more data on the morbidity and possibly more associations between hospitalisations and mortality. This study does not answer the question if homelessness in itself is a risk factor of death or if the risk is increased by the factors leading to homelessness such as psychiatric morbidity and lack of capacity to handle crisis.
Our study can be rightfully criticised for not having a large sample. This affects the lack of power of the predictors of mortality as well as makes it impossible to calculate sHR for all causes of death, having a bigger sample form a geographically larger area would have given more information. Then again, our study population consists of all male shelter users in Helsinki in 2004. Using personal identification codes enabled accurate linking of the data from the used registers. The high quality of the Finnish registers29 and the Finnish tradition of performing medicolegal autopsies30 strengthened our study, and as a result, we had only few deaths due to unknown cause. A weakness in our study set-up included only men: we have no data on the mortality of female homeless. By using a shelter population, we also did not have information on those homeless that sleep rough, in temporary lodging or institutions. However, considering the harsh climate in Finland, very few actually sleep outdoors all year around,31 and since our sample covered the whole calendar year, it is likely that those sleeping outside during warmer months would have entered the shelter at some point during the cold winter. Although it would have been interesting to compare the homeless shelter population with the homeless in institutions and temporary lodgings, it was impossible to do as there are no representative registers of these. We also do not know the length of homelessness prior or post baseline. However, we can assume that many of those here classified as homeless moved into some form of supported housing during the long follow-up. Despite this, their death rate remained high, and after 10 years, almost half had died.
We conclude that being homeless to the point of having to use shelter services poses a serious threat to life. Hence, shelters should be provided with good social and healthcare support to actively help this high-risk population.
What is already known on this subject
Homeless people are at risk of premature death from diseases and medical conditions as well as from external causes. Substance use disorders, non-immigrant background and extended homelessness are previously identified predictors of death among homeless.
What this study adds
Using a matched control group and modern statistical survival methods, in a competing risks framework, we could produce more exact estimates on all-cause and cause-specific mortality than previous studies. We also found that not being employed or married and having only basic level education were significant predictors of death in the control group, but these factors had no relevance in predicting death for homeless. These results suggest that the depth of segregation being homeless entails over-rides the protective effects of education, marriage and employment acquired earlier.
Acknowledgments
The authors thank the staff at City of Helsinki and Sigrid Rostén for helping to gather the data, the National Institute for Health and Welfare for technical support and all funders.
References
Footnotes
Contributors JGE, AS-A, HK and PH designed the study. AS-A collected the data. HK and AS-A performed the analysis. PH, JGE, MG and KW contributed to the interpretation of the results and critical revision of the manuscript. AS-A drafted the manuscript, and all authors contributed to and approved the final version.
Funding The study has been funded by Samfundet Folkhälsan, Finnish Medical Association (Finska läkaresällskapet), the Wilhelm and Else Stockmann's foundation and the Finnish Foundation for Alcohol Studies.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Ethics approval for this study was granted by the ethics committee of the Hospital district of Helsinki and Uusimaa (HUS), and research permits were obtained from all the register keepers in the study, respectively. The Data Protection Ombudsman gave his statement before the study data were created, as requested by the national legislation on data protection.
Provenance and peer review Not commissioned; externally peer reviewed.