Article Text

Abstract
Background Ample evidence has shown that early-life social conditions are associated with mortality later in life. However, little attention has been given to the strength of these effects across specific age intervals from birth to old age. In this paper, we study the effect of the family's socioeconomic position and mother's marital status at birth on all-cause mortality at different age intervals in a Swedish cohort of 11 868 individuals followed across their lifespan.
Methods Using the Uppsala Birth Cohort Multigenerational Study, we fitted Cox regression models to estimate age-varying HRs of all-cause mortality according to mother's marital status and family's socioeconomic position.
Results Mother's marital status and family's socioeconomic position at birth were associated with higher mortality rates throughout life (HR 1.18 (95% CI 1.12 to 1.26) for unmarried mothers; 1.19 (95% CI 1.12 to 1.25) for low socioeconomic position). While the effect of family's socioeconomic position showed little variation across different age groups, the effect of marital status was stronger for infant mortality (HR 1.47 (95% CI 1.23 to 1.76); p=0.04 for heterogeneity). The results remained robust when early life and adult mediator variables were included.
Conclusions Family's socioeconomic position and mother's marital status involve different dimensions of social stratification with independent effects on mortality throughout life. Our findings support the importance of improving early-life conditions in order to enhance healthy ageing.
- Life course epidemiology
- Lifecourse / Childhood Circumstances
- INEQUALITIES
- MORTALITY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Socioeconomic inequalities in mortality are the most widely documented evidence of social disparities in health globally.1 The recognition that health is not only the result of current circumstances, but rather of multiple processes operating across the entire life course, has led scholars to investigate the association between early-life socioeconomic conditions and adult mortality.2–10 A systematic review11 shows that socioeconomic characteristics in childhood are important predictors of all-cause mortality in later life, although the association becomes attenuated in models adjusted by adult socioeconomic position. This has led to the conclusion that measuring socioeconomic characteristics at only one point in time is not enough to capture the full extent of socioeconomic inequalities in health.4
However, there are still gaps that need to be explored to better understand the role of childhood socioeconomic conditions on mortality. Studies in this field are usually conducted on participants recruited after reaching adulthood,12 with childhood information obtained either from census data (ie, not measured at birth for all participants),3 ,5 or else from interviews conducted later in childhood2 or during adulthood,13 the latter of which has been shown to underestimate the true association.14 Furthermore, most studies are performed in relatively young cohorts,2–4 ,6 ,15 which does not allow tracking of the effects beyond premature mortality (ie, after 70 years of age)16 or investigation of potential variation in the strength of the effect across different age intervals. It is necessary to fill this gap in order to determine how long the impact of childhood socioeconomic conditions lasts throughout the life course.
Apart from methodological limitations, most epidemiological studies in this area focus only on childhood socioeconomic conditions, for example, parental occupation or other proxies for material living standards. Other potentially important social dimensions are generally overlooked. Such is the case for mother's marital status, which can lead to social vulnerability due to the stigma of illegitimacy or to other disadvantages such as reduced material resources or the lack of parental involvement.17–19 Even in contemporary settings, having an unmarried mother is associated with adverse health and social outcomes in the child and following generations.20 ,21
Several mechanisms (material and psychosocial) have been put forward in the literature to explain how socioeconomic inequalities in childhood translate into disparities in mortality later in life; and different life-course models have been suggested to describe how such mechanisms might operate (critical, accumulation and sensitive periods).22 Thus, childhood socioeconomic conditions could directly influence adult mortality by altering the susceptibility to develop a particular disease already in the uterus through fetal programming (ie, a critical period effect).23 Alternatively or additionally, childhood socioeconomic conditions could be linked to adult mortality indirectly through a chain of cumulative disadvantages that materialise in different life-course trajectories, the so-called ‘unhealthy life careers’24 (eg, childhood malnutrition contributes to poor cognitive abilities, which leads to poor school performance, which in turn affects job opportunities and later health).24 ,25
In this paper, we study the long-term effects of early-life socioeconomic and social conditions (measured via familial occupational position and marital status) on all-cause mortality in a cohort of 11 868 participants followed throughout almost their entire lifespan. Our specific aims are to assess (1) the effect size across age-specific intervals and (2) the remaining effect after the inclusion of early-life health characteristics and adult socioeconomic characteristics (mediators).
Methods
Study population
Our study is based on the Uppsala Birth Cohort Multigenerational Study (UBCoS Multigen) (http://www.chess.su.se/ubcosmg/), which contains all live births at the Uppsala University Hospital, Sweden, between 1915 and 1929.26 ,27 The follow-up was initiated at birth and continued until death, emigration or 31 December 2009, whichever was earliest. From a total of 14 192 live births, we excluded multiple births (n=444), as their growth rate is reduced in the final trimester.28 We then further excluded 11.4% of singleton births because of missing data on birth weight (n=101), gestational age (n=398), parity (n=1), maternal age (n=1), marital status (n=29) or parental occupation (n=1093). Among those with missing data on parental occupation were 723 offspring of mothers whose occupation was listed as ‘house-daughter’, which is effectively a measure of marital status (house-daughters were typically single women living with their parents at the time of the birth of their child). We also excluded participants if the recorded gestational age was below the biological viability threshold of 22 weeks (n=2) or if the individual could not be traced after their birth (n=255). The main analyses are therefore based on a sample of 11 868 participants.
In subanalyses to assess the effect of adult socioeconomic characteristics, we excluded those participants who did not survive to the age of 55 years (n=2092; 18%). This decision was made to ensure that we have adult socioeconomic information for all individuals since the information comes from Census data (1960 and 1970). Also, we excluded observations with missing data on education (n=36), occupation (n=191) and income (n=218) in adulthood. The total sample to study the effect of socioeconomic conditions in adulthood comprises 9441 participants.
Childhood characteristics
Table 1 presents the explanatory variables examined. Birth weight was classified into <3000, 3000–3999 and ≥4000 g. Gestational age was categorised into preterm (<37 gestational weeks), term (37–41 weeks) and post-term (≥42 weeks). Mother's age at the index child's birth was categorised into four groups: ≤24, 25–29, 30–34, and ≥35 years old. Parity was assessed as 1, 2, 3 and ≥4, and year of birth was categorised into three groups: 1915–1919, 1920–1924, and 1925–1929.
Characteristics of the analysed population, number and proportion of deaths, and death rates
Socioeconomic variables
Familial socioeconomic information at the time of birth was derived from the Swedish socioeconomic classification scheme,29 using father's occupation (80%) or, if not reported, mother's occupation (20%).30 This was categorised into high (higher and intermediate non-manuals, entrepreneurs and farmers), middle (lower non-manual and skilled manuals) and low (unskilled manuals). Mother's marital status at the index child's birth was classified into married and unmarried (single/divorced/widowed).
Adult socioeconomic characteristics were conceptualised as potential mediators in our analyses. Occupation in adulthood was obtained from the 1960 Census. We categorised this variable into disadvantaged (manual workers, agricultural workers, self-employed individuals, students, or other non-working) and advantaged (managers and professionals, non-manual workers and the military). Education was categorised into lower (≤10 years of education) and higher (>10 years of education). Marital status of the cohort member was categorised into married and unmarried (single/divorced/widowed) based on data collected in 1960. Family disposable income was obtained from the 1970 Census and analysed in tertiles.
Statistical analysis
We fitted Cox regression models using age to define the timescale. We were guided by our interest in assessing how the effects of marital status and family socioeconomic position varied across different age intervals. The models were stratified by age using the following bands: <1, 1–19, 20–54, 55–64, 65–74, and ≥75. This allowed us to derive estimates of age-band-specific HRs for all-cause mortality, with 95% CIs. All models were fitted with robust SEs by taking into account the clustering of siblings within mothers. We initially fitted minimally adjusted models including the study participant's sex and birth year to assess the effect of familial socioeconomic position on mortality and of marital status on mortality. Thereafter, we expanded the corresponding models by including partial adjustments (birth weight, gestational age, parity and maternal age) in order to better assess the direct effect of familial socioeconomic position and marital status, respectively, on mortality. Following the literature on fetal programming, we included birth weight and gestational age in this model, as these variables could be in the pathway between childhood socioeconomic condition and mortality (especially for cardiovascular-related cause mortality).31 Finally, we further expanded these models by mutually adjusting for family's socioeconomic position and marital status. We systematically assessed whether the association between socioeconomic characteristics and mortality was modified by the study participants’ sex as well as the possible interaction between family's socioeconomic position and mother's marital status in their effect on mortality. Interactions were assessed using the Wald test.32
In order to better illustrate age-specific effects, we displayed the age-varying HRs and their 95% CIs in forest plots. This is a graphical representation of the estimations at each age band with an overall pooled effect size estimated using random effects meta-analysis. It includes a statistic (I2) that measures the percentage of between-age true heterogeneity from the total observed variation. Thus, this approach allows us to formally test effect modification by age intervals, that is, to identify true variation (as opposed to random error) in effect size across age bands. I2 statistics lie between 0% and 100%. The following tentative thresholds have been proposed33 to interpret the levels of heterogeneity: low (I2 between 25 and 50%), moderate (I2 between 50% and 75%), and high (I2≥75%).
All analyses were performed using Stata, V.11, software (Statacorp, LP, College Station, Texas, USA).
This study was approved by the Regional Ethics Committee in Stockholm.
Results
During the 813 729 person-year (pyar) follow-up (average, 68.56, median 80), 8016 individuals died. Table 1 depicts the distribution of the number of participants at risk, deaths and death rates per 1000 pyar by different levels of the explanatory variables. The offspring of unmarried mothers as well as the offspring from families with a low or middle socioeconomic position had higher death rates (≈10/1000 pyar). This trend persisted into adulthood; death rates were higher (between 24 and 30/1000 pyar) in all unfavorable socioeconomic categories such as basic education, disadvantaged socioeconomic position and unmarried. Table 1 also shows variations in mortality rate according to characteristics such as sex, birth weight and parity, as reported by us in previous analyses (SP Juárez, A Goodman, B DeStabola, et al. Perinatal health and all-cause mortality: a sibling analysis using the Uppsala Birth Cohort Multigenerational Study. Under review).
Figure 1A, B shows the survival curves by early-life marital status and family socioeconomic position. The adverse effect of being the offspring of an unmarried mother (A) and, to a lesser extent, of being born to a family of low (vs high) socioeconomic position (B) is systematically observed at all ages (p=0.59 for heterogeneity). The effect of being born in a family of middle (vs high) socioeconomic position is likewise observed at all ages (p=0.39 for heterogeneity).
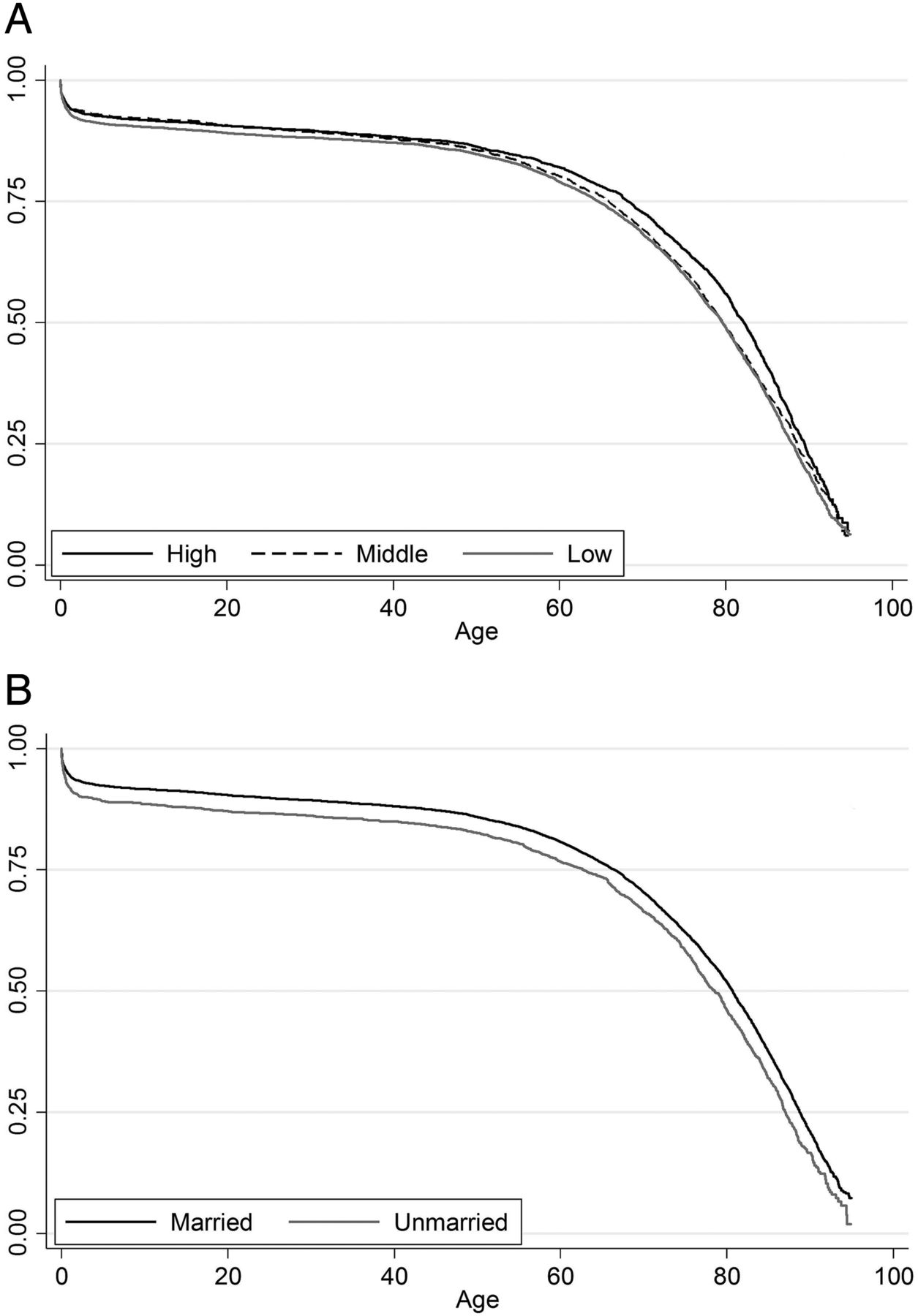
Kaplan-Meier survival curves by family's socioeconomic position (A) and mother's marital status (B) and from the Uppsala Birth Cohort Multigenerational Study, born 1915–1929.
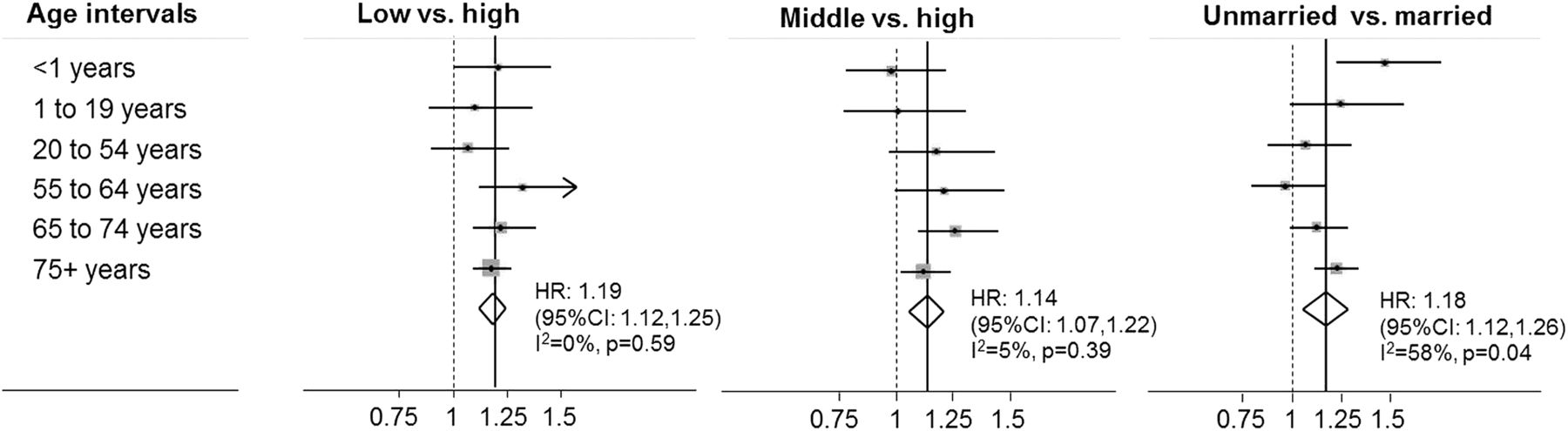
Table 2 shows the association between childhood social characteristics (mother's marital status and family's socioeconomic position) and mortality in models adjusting for different sets of covariates. Regardless of model specifications, being a newborn of an unmarried mother and in a family of low and middle socioeconomic position is associated with higher mortality rates. When examining these associations by age-specific intervals (figure 2), only maternal marital status showed some evidence (p=0.04) of moderate heterogeneity between age intervals (I2=58%). Specifically, maternal marital status was significantly associated with higher mortality rates during the first year of life (HR 1.47, 95% CI 1.23 to 1.76) and after 75±years of age (HR 1.23, 95% CI 1.12 to 1.34) (see online supplementary table S1). This possible heterogeneity suggests that the pooled effect size in table 2 should be treated with some caution, although given that the evidence of heterogeneity is marginal, we have still chosen to present the pooled effect size to allow comparison with the effect of socioeconomic position and with other studies. The results for marital status with respect to heterogeneity by age remain after the inclusion of early-life mediator factors (birth weight, gestational age, parity and maternal age). The inclusion of adult socioeconomic characteristics among those individuals who survived at 55 years of age (80%) did not substantially change the results (see online supplementary table S2).
Association between childhood social characteristics and all-cause mortality: age-varying HRs and 95% CIs
{kind=link}
{kind=link}
Random-effect meta-analysis of the effect of family's socioeconomic position and marital status on mortality by age intervals.
No interactions were found between marital status and child's sex or between marital status and family socioeconomic position in any age band (p value >0.05).
Discussion
Summary of the results
Unfavourable family socioeconomic characteristics at birth and being born to an unmarried mother are associated with higher mortality rates. The effect of family socioeconomic characteristics on all-cause mortality was robust and did not show appreciable variation in strength across age-specific analyses. However, mother's marital status showed effects of varying strength depending on the age interval studied. The offspring of unmarried mothers had a higher risk of infant mortality compared with the overall effect. The effects of early-life social characteristics on adult mortality persist after the inclusion of adult socioeconomic characteristics (occupation, education and income) and marital status. These findings suggest that the effect of early-life social conditions lasts across the life course. No interactions were found between gender and mother's marital status or family's socioeconomic position in their effect on mortality.
Originality
To the best of our knowledge, this is the first study that investigates the effect of family's socioeconomic position together with mother's marital status at birth by age at death within an almost complete representative cohort. In contrast to most previous studies on early-life socioeconomic inequalities in mortality, we included mother's marital status as a social variable and explored its effect on mortality before and after the inclusion of family socioeconomic position. We found that mother's marital status and family's socioeconomic position have independent effects on mortality in mutually adjusted analyses, and without any evidence of an interaction between them. This finding suggests that family's socioeconomic position and mother's marital status involve different dimensions of social stratification with specific effects on mortality throughout life.
Consistency with other research
Since we did not find previous studies with similar designs and settings, the comparison of the results can only be partial. Consistent with previous studies,2 ,4 ,5 ,34 we found an association between childhood socioeconomic position and mortality. In line with most studies,2–4 ,6 but not all,5 ,35 the effect of early-life social characteristics on all-cause mortality was not fully mediated by adult socioeconomic characteristics. Our findings therefore add further evidence to the observation that only measuring adult socioeconomic characteristics will not accurately capture the full extent of socioeconomic differences in mortality.4
Our findings are consistent with one study in the UK2 that showed higher death rates at age 26-54 among manual workers born in 1946 and with another study in Sweden3 that showed higher death rates at age 25–40 among manual workers born between 1946 and 1955, although our results differ from one study from England and Scotland13 that did not find any effect of parental occupation on mortality at ages 35–64 among individuals born between 1937 and 1939. The comparison between cohorts from similar contexts does not support the thesis that socioeconomic inequalities in mortality might not have been observed before World War II due to the combination of high virulence of diseases where all social groups were equally exposed together with the inefficacy of medical treatments.36
The effect of marital status is consistent with the results of two further studies, one on infant mortality34 and the other on mortality over 50 years of age.37 Our results are also consistent with an earlier study using the same data but with a shorter follow-up of these data which found that there was a lower probability of reaching 80 years of age among the offspring of single mothers.19
Strengths and limitations
This study is based on a representative,38 nearly complete cohort of individuals followed during almost their entire lifespan. This data material allowed us to estimate age-varying HRs and also to study the effect of childhood socioeconomic conditions on mortality at old age, whereas previous studies could only focus on younger groups.2 ,3 In contrast to other studies,3–5 ,13 information on socioeconomic conditions was measured for all participants at the time of birth, which increases comparability among the participants. Unlike past research,2–5 we additionally explored the effect of marital status and its interaction with family socioeconomic position.
Owing to the small sample size, we could not study the children of divorced (n=21, 0.18%) and widowed (n=59, 0.50%) women as a separate group. We acknowledge that the grouping of children of single, divorced and widowed women together may introduce heterogeneity. Likewise, since we only have information on marital status, we cannot identify those mothers who were cohabiting with the child's father or otherwise receiving his support. Another potential source of heterogeneity lies in the fact that family's socioeconomic position and mother's marital status were measured at only a single point in time (the child's birth), meaning that we are unable to examine the dynamics of these over time. This might especially be a problem if the cumulative life-course model is the one that best describes the association between childhood conditions and adult mortality.
A further limitation is the lack of information on parental education and income, which has been shown to be complementary information that captures different dimensions of social stratification.39 In addition, although our study was well powered at older ages, we were forced to use relatively broad age intervals at younger ages (eg, 1–19 years).
In this study, we did not conduct a detailed mediation analysis, and so are unable to examine the underlying mechanisms of the effects we observed. Insofar as the inclusion of birth weight and gestational age in our study did not substantially change the strength of the association, it seems likely that these are not important mediators of the effects observed. However, we lacked data on other plausible mediators such as cognitive abilities or personality, and therefore are unable to examine how far these might lie on the pathway between early-life social conditions and mortality.
Finally, in contrast to other cohort studies,2 ,5 the Uppsala Birth Cohort was relatively less affected by World War II. Nonetheless, Sweden was not exempt from experiencing other ‘external shocks’; the Spanish flu (1918–1920) may have influenced older participants of the cohort, and the Great Depression (1929–1939) may have particularly influenced individuals born in the 1920 as the crisis took place during their early childhood. Concerning migration, we did not expect serious distortions as the proportion of out-migrants was only 1.42%. This might be due to the fact that Sweden, unlike other countries, such as the UK, started expanding its social security system from this time,40 thereby buffering any adverse effects of the crisis.
Implications for future research
Using a representative and an almost complete cohort, our study confirms that early-life socioeconomic conditions have a long-standing effect on all-cause mortality, regardless of adult socioeconomic characteristics. Further studies in other settings should confirm this pattern and elaborate on the mechanisms through which being born to a family of high socioeconomic position and/or a married mother might protect individuals from premature death.
Our findings are based on all-cause mortality, a summary measure of health at the population level. Although many plausible biological and social pathways for a long-term effect of early-life social conditions on later health have been proposed, further studies looking at specific causes of death might better elucidate the underlying disease-specific mechanisms. Previous studies have, for example, found that the association between parental social characteristics and all-cause mortality is predominately driven by cardiovascular disease5 ,7 and stroke in particular.13
Studies looking at early-life socioeconomic effects on adverse health outcomes later in life should also consider family composition and mother's marital status. Our findings suggest that marital status has a specific effect on mortality, that is not explained or modified by the role of family socioeconomic position. Further studies should confirm this result and assess the specific mechanisms through which different social characteristics (inasmuch as they represent different dimensions of social stratification) influence health and mortality differently across ages.
Conclusion
This study suggests that both mother's marital status and family's socioeconomic position in early childhood have an effect on mortality across the lifespan. The effect of marital status is strongly associated with mortality during the first year of life. These findings support the importance of improving early-life conditions in order to enhance healthy ageing.
What is already known on this subject
Studies have shown that socioeconomic characteristics in childhood are important predictors of all-cause mortality in later life. However, studies in this field are usually conducted in relatively young cohorts, and have not investigated the potential for variation in the strength of the effect across different age intervals.
What this study adds
Our Study is based on an exceptional data set that follows a cohort of individuals born between 1915 and 1929 across their lifespan. This material allowed us to assess, for the first time, the effect of early-life social characteristics on mortality at different age intervals from birth to old adult ages.
This study shows that the adverse effect of social conditions is associated with a lower survival at all ages. This early-life effect extends to other categories such as marital status that conferred (and to some extent still confers) a socially disadvantaged position in society.
The effect of family socioeconomic position did not show appreciable variation in the strength of the association across age-specific analyses; however, marital status shows a stronger effect for infant mortality.
Our findings led to the conclusion that only measuring adult social characteristics does not accurately capture the full extent of socioeconomic differences in mortality. This evidence supports the importance of improving early-life conditions in order to enhance healthy ageing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors All authors made substantial contributions to the conception and design of the study. The study was conceived by IK and SPJ. The analyses were conducted by SPJ. AG advised on the design and implementation of the meta-analyses. SPJ drafted the manuscript and all the authors revised and made critically important contributions. All the authors approved the final version of the manuscript.
Funding This work was supported by Vetenskapsrådet (VR#2013-5104, PI Koupil, VR #2013-5474, PI Rignell-Hydbom) and FORTE (# 2013-1084, PI Koupil, #2014-2693, PI Koupil, #2006-1518, PI Lundberg).
Disclaimer The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Ethics approval Regional Ethics Committee in Stockholm.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The Uppsala Birth Cohort Multigeneration Study (UBCoS Multigen) is a study established at the Centre for Health Equity Studies (CHESS) with the aim of investigating the life course and intergenerational determinants of social inequalities in health. For further information or enquiries about access to data, please contact the principal investigator IK at ilona.koupil@chess.su.se.