Article Text

Abstract
Background A reduction in sex ratio at live birth has been proposed as a sentinel health indicator that can be used to monitor the health of populations.
Objective To test the hypothesis that a lower sex ratio is associated with adverse national population health using the prevalences of HIV and tuberculosis as measures of societal well-being.
Methods An ecological study design using routinely collected data and adjusting for potential confounding factors.
Results The mean global sex ratio was 1.05. There was marked heterogeneity in the sex ratio between different global regions (p<0.0001). Those regions with the highest prevalences of HIV infection had lower sex ratios, with the value for the highest quartile being 0.022 (95% CIs CI 0.013 to 0.031) lower than the lowest quartile. Similarly, those areas with the highest quartile of tuberculosis infection had a sex ratio of 0.016 (95% CI 0.004 to 0.028) lower than those in the lowest quartile. Similar results were observed in a subgroup analysis limited to countries from the African continent.
Conclusions The data are consistent with the hypothesis that a reduced sex ratio at live birth is a potential sentinel health indicator of lower population health. However, these data do not demonstrate either a casual relationship or reveal any biological mechanisms that may account for these observations.
- Sex Ratio
- Population Health
- Tuberculosis
- Malaria
- Epidemiology
- Obesity
Statistics from Altmetric.com
The sex ratio of males to females at live birth is normally approximately 1.05.1 ,2 Davis et al2 reported that the sex ratio at live birth decreased in the second half of the 20th century in Denmark, the Netherlands, Canada and the USA and speculated that this may represent a sentinel health indicator that may be of use in identifying environmental changes that modify population health. Although there have been many studies looking at associations between sex ratio and environmental exposures such as hepatitis B virus,3 psychological distress,4 concurrent conflict and wars,5–7 recent earthquakes,8 ambient temperature,9 economic stress10 and exposure to environmental chemicals,11 no consistent data exist to provide a single biological mechanism for this proposed association. In 1973, Trivers and Willard12 suggested that natural selection may favour parental ability to adjust the sex ratio based on ability to support the offspring and used animal data to demonstrate that as the maternal condition declines, the adult female produces a lower ratio of males to females. However, reliable data to test the hypothesis that environmental exposures impact on the sex ratio in humans at live birth at the population level relies on opportunistic studies utilising observational data from comparative studies.
HIV/AIDS and tuberculosis (TB) represent two infections that have a wide heterogeneous distribution between different countries and may be considered as examples of environmental factors which impact on both individuals and populations. As a consequence, this provides an opportunity to test the hypothesis that these environmental stressors are associated with a reduction in the sex ratio at live birth in these societies. We have used an ecological study design to study the association between the two exposures of national prevalence of HIV/AIDS and TB with the sex ratio at live birth, using all recent global data available and adjusting for measures of economic activity,13 latitude14 and malnutrition15 as previously identified potential confounding factors. We also conducted a subgroup analysis to test this hypothesis using data from of the African countries.
Methods
Study population
We used data from all countries with available data. Data were obtained from three demographic databases including the WHO Global Observatory database,16 the United Nation database ‘UNdata’17 and the Central Intelligence Agency world factbook.18 We used the most recent available data for all variables of interest (2005–2010). The raw data used in these analyses are presented in an online supplement.
Variables of interest
The outcome variable for the study was the sex ratio at live birth. This is defined as the number of male babies born per 100 female babies in an annual population in 2010. The two exposures of interest were the national prevalences of HIV/AIDS and TB in 2009. These data were collected at country level through health facilities or national studies monitored by national health institution before being aggregated in the WHO Observatory database.
Other variables were considered as a priori confounding factors based on pre-existing literature. These included national per capita Gross National Product using the most recent 2009 annual estimates,19 latitudinal distance from the equator, which has also been associated with sex ratio at live birth,14 and the national prevalence of malnutrition, which may also modify the sex ratio at live birth.15 All confounding factors were coded in quartiles.
Data analyses
We used an ecological study design. The primary analysis used the global data set, and a subgroup analysis was subsequently completed of the countries from the African continent. We used the analysis of variance (ANOVA) test to statistically examine differences between the sex ratio at live birth for the different global regions.
The Spearman rank correlation test was carried out to initially measure the associations between the sex ratio at birth and exposure prevalences. In addition, linear regression was used to study the association between the sex ratio at birth and each exposure variable and to adjust for potential confounding factors. The likelihood ratio test was used to determine if the association between exposures and outcome variables were continuous or categorical. As the likelihood ratio test indicated non-linear associations between the outcome and both exposure variables, the exposure variables were modelled as quartiles. As the relationship between the prevalences of HIV/AIDS and TB were highly co-linear (r =0.50, p<0.0001), we were unable to model both HIV and TB disease prevalence in the same model. The data were analysed using STATA V.11 statistical software (StataCorp, Texas, USA).
Results
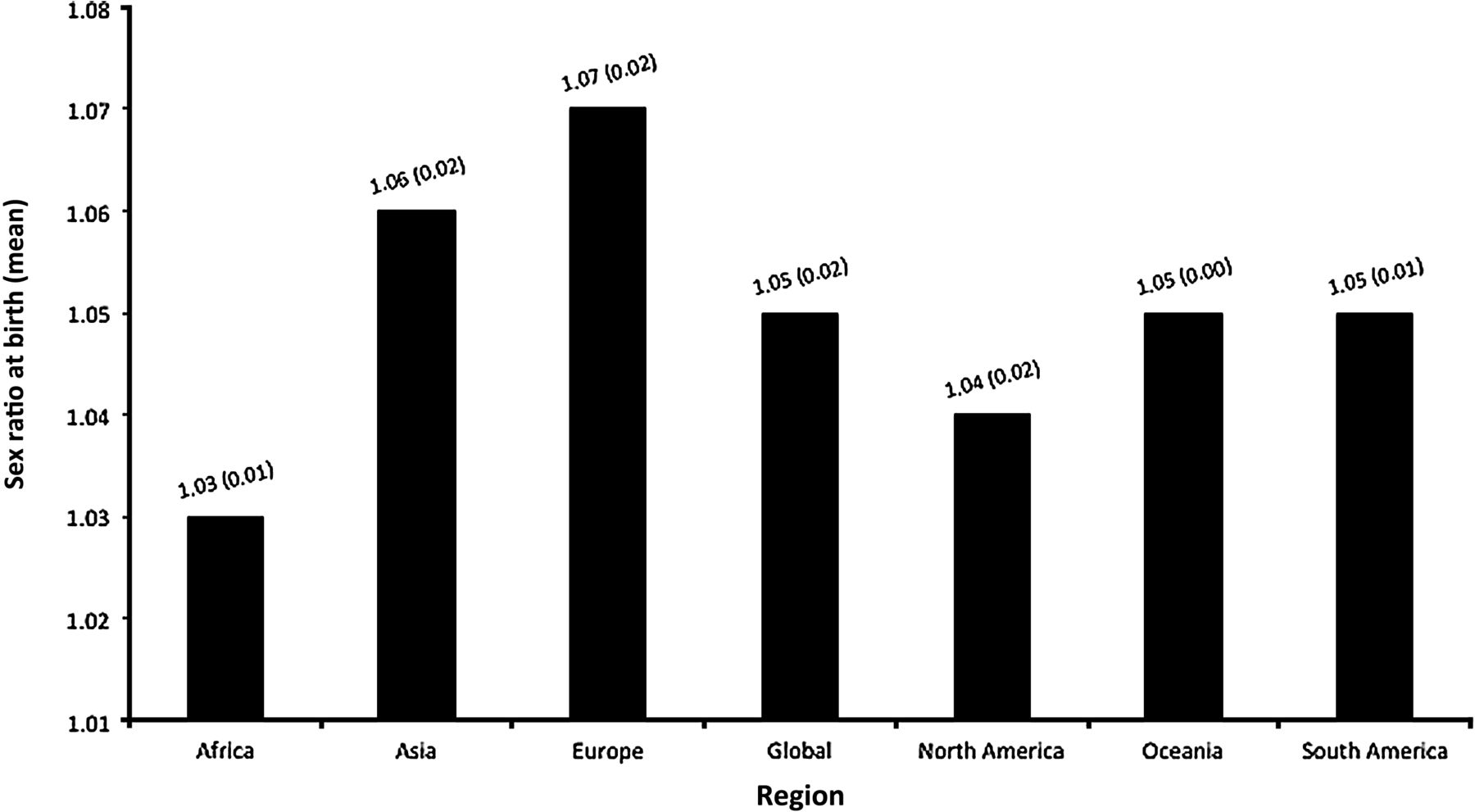
Data were available for 184 countries globally of which 53 were from the African continent. The global sex ratio at live birth was 1.05 (SD 0.02) with significant differences between regions (p<0.0001, ANOVA test). The mean sex ratio at birth for each region is presented in figure 1 and varied from a low of 1.03 (SD 0.01) in the African continent to 1.07 (SD 0.02) in Europe.

Mean sex ratio at birth (SD) by region.
Global analysis
Table 1 shows the median prevalence of HIV/AIDS and TB stratified by world regions. The median HIV/AIDS prevalence was highest in the African continent (2.5%; IQR 0.9%–5.3%) and lowest in Asia (0.1%; IQR 0.1%–0.2%), Europe (0.1%; IQR 0.1%–0.3%) and Oceania (0.1%; IQR 0.1%–0.5%). Similarly, the African continent had the highest prevalence of TB (397 cases per 100 000 people; IQR 191–562 cases per 100 000 population) and Europe had the lowest prevalence of TB (15 cases per 100 000 people; IQR 8–47 cases per 100 000 people).
Prevalence of HIV/AIDS and tuberculosis (TB) by global regions
For the global study population, there was a significant negative correlation (r=−0.58, p<0.0001, Spearman test) between the sex ratio at birth and national HIV/AIDS prevalence. A similar negative relationship (r=−0.48, p<0.0001) was also observed between the sex ratio at birth and the national TB prevalence. As likelihood ratio testing demonstrated a non-linear association between the sex ratio at live birth and both prevalence of HIV/AIDS (p=0.019) and TB (p<0.001), subsequent analyses used quartiles to further explore these relationships.
After adjustment for the potential confounding by per capita Gross National Product, latitude and malnutrition, significant associations remained between both prevalences of HIV/AIDS and TB with sex ratio at live birth (table 2). Populations with the highest quartile of HIV/AIDS prevalence had a reduced sex ratio at birth compared with those with the lowest quartile −0.022 (95% CIs −0.031 to −0.013). Similarly, populations with the highest quartile of TB prevalence had a reduced sex ratio at birth compared with those with the lowest quartile −0.016 (95% CI −0.028 to −0.004).
Association between the human sex ratio at birth and prevalence of HIV/AIDS and tuberculosis (TB): global analysis
Analysis of countries from African continent
Figure 2 summarises the variation in the sex ratio at birth between the different subregions of Africa that varied significantly between regions (p<0.0001, ANOVA). The sex ratio at live birth was 1.03 in all subregions except Northern Africa, which had a mean value of 1.05 (SD 0.01).

{kind=link}
{kind=link}
Mean sex ratio at birth (SD) by African subregion.
The sex ratio was inversely associated with prevalence of both HIV/AIDS and TB in the countries from the African continent (Table 3). After adjustment for potential confounding factors, the sex ratio was lower in populations with the highest quartile of HIV/AIDS prevalence compared with those with the lowest quartile (difference of −0.009, 95% CI −0.018 to −0.0005). Similarly, a reduction in the sex ratio at birth was also observed in those populations with the highest quartile of TB prevalence compared with those with the lowest quartile (difference −0.009, 95% CI −0.017 to −0.002).
A post hoc analysis of the non-African countries did not demonstrate any association between sex ratio and either prevalence of HIV or TB in quartiles, after adjusting for the confounding factors.
Discussion
Our data demonstrate that in the early 21st century, there are marked differences between different regions in the sex ratio at live birth. In countries with a high prevalence of either HIV/AIDS or TB, there is a lower sex ratio at live birth, and these observations are also present in the subgroup analysis restricted to countries from the African continent. This phenomenon is observed with both infectious diseases and persists after adjustment for potential confounding environmental factors. These associations are consistent with the hypothesis proposed by Davis et al2 that sex ratio at live birth may be a sentinel measure for the health of populations, and this is an important area of study, as environmental exposures that modify this measure will influence the demographic structure of future generations.
Strengths and weaknesses
The strength of our analysis is that it tests a pre-existing hypothesis using a global data set of routinely collected data from 184 countries with the capacity to adjust for potential confounding factors such as economic activity, prevalence of malnutrition and latitude. The availability of data from 53 countries from the African continent also permits a subset analysis, which permits further testing of the associations observed within a slightly less heterogeneous group of nations.
Our analysis has a number of limitations that require consideration. The ecological study design is one that has a variety of methodological problems compared with other epidemiological study designs.20 However, when testing the hypothesis that a population-based stressor may impact on a population-based outcome, it may be the best study design available to identify major population-level determinates of disease.21 However, the use of routinely collected data makes the generalisability of any associations observed restricted to comparisons within countries, and other study designs will be required to explore these associations within national borders. The associations that we have observed between both high prevalences of HIV/AIDS and TB and a low sex ratio at live birth are not evidence of a causal relationship, although we cannot exclude this possibility for one of the exposures. There are other factors in common between countries with a high prevalence of both of these infectious diseases, which we were unable to adjust for in our analyses that may shed more light on the causal pathways involved. Such factors include the genetic/ethnic mixture of the national populations,22 ,23 the preference of certain populations for male offspring,24 ,25 increased paternal age26 and local geography, which will substantially modify the environment. It is possible that some of these exposures that are intrinsic to or associated with regional cultures may explain some of the associations that we report, and future studies of environmental factors that may modify sex ratio would be enhanced by consideration of both the ethnicity of individuals concerned and cultural factors including religious beliefs. The nature of our data set does not permit these factors to be considered in this analysis, although one study design that may increase understanding of the associations of interest could be a time series analysis of national data over the period that HIV and TB prevalence changed. The absence of an association between either HIV or TB prevalences and the sex ratio from the non-African countries was not surprising, as the range of prevalences for both infectious diseases in these regions were relatively low, thus limiting the power of these analyses.
To our knowledge, this is the first study to present data on the association between the prevalence of either HIV/AIDS or TB and the sex ratio at live birth. There have been many studies utilising routinely collected data and examining the association between acute and chronic environmental exposures and sex ratio at live birth. Our data are consistent with an early paper by Willard and Trivers12 who used data from mammals to speculate that the sex ratio at live birth decreases in times of scarcity, another challenge to the health of populations. However, they are less consistent with the observations that the sex ratio increases during times of extended war6 and famine15 and also appears to be increased in individuals with hepatitis B infection.3 As these exposures are indisputably population stressors, it is clear that untangling the relationships between exposures and the human sex ratio is a challenging area of investigation, and the nature, duration and intensity of the exposures may all be factors that warrant consideration in future studies. Reports that higher levels of psychological stress4 and exposure to severe life events27 during early gestation are associated with a lower sex ratio at live birth may be relevant in providing a potential biological mechanism to explain our observations.
From a practical perspective, as well as suggesting that the sex ratio at live birth may have potential as a sentinel health indicator, our observation of 1%–2% decrease in sex ratio in countries with a high prevalence of HIV/AIDS and TB has implications for the demographic structure of these countries in the future, particularly if these patterns of lower levels of male birth are compounded over decades or longer. This is a relatively large size of association that is of a similar magnitude to the change reported in economically developed countries by Davis et al2 over the second half of the 20th century.
What is already known on this subject
-
It has been hypothesised that sex ratio at live birth can be used as a sentinel measure of population health.
-
No studies have tested this hypothesis.
What this study adds
-
Sex ratio at live birth is inversely associated with both the prevalences of HIV and TB, with a higher prevalence of either infection being associated with an increase in women compared with men.
-
These data do not demonstrate a casual association but are consistent with the hypothesis that sex ratio at live birth is a measure of societal well-being.
Association between the human sex ratio at birth and prevalence of HIV/AIDS and tuberculosis (TB): African analysis
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online Supplementary Data
Footnotes
-
Contributors The hypothesis was developed by AWF, and AS did the data collection and data analysis. Both authors drafted and wrote the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement We are submitting all the raw data as an online supplement.