Article Text

Abstract
Debates have raged in development for decades about the appropriateness of participatory approaches and the degree to which they can be managed, scaled and measured. The Avahan programme confronted these issues over the last 7 years and concludes that it is advantageous to manage scaled community mobilisation processes so that participation evolves and programming on the ground is shaped by what is learnt through implementation. The donor (Bill & Melinda Gates Foundation) and its partners determined a standard set of programme activities that were implemented programme-wide but evolved with input from communities on the ground. Difficulties faced in monitoring and measurement in Avahan may be characteristic of similar efforts to measure community mobilisation in a scaled programme, and ultimately these challenges informed methods that were useful. The approach the programme undertook for learning and changing, the activities it built into the HIV prevention programme, and its logic model and measurement tools, may be relevant in other public health settings seeking to integrate community mobilisation.
- Community participation
- community mobilisation
- HIV prevention
- female sex workers
- evaluation methodology
- organisational development
- socio-economic
- social inequalities
- social science
- social capital
- sexually trans dis
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Community participation
- community mobilisation
- HIV prevention
- female sex workers
- evaluation methodology
- organisational development
- socio-economic
- social inequalities
- social science
- social capital
- sexually trans dis
Background
Among the topics reflected on with 7 years of learning from implementing a scaled HIV prevention programme in India are: the challenge and benefits of facilitating meaningful participatory processes, incorporating effective monitoring, and responding to change through flexible management. The operational experience from Avahan suggests that a community mobilisation approach can be ethical, providing space for communities to reshape interventions to better serve their needs, while being a deliberately managed, measured and scaled process. The monitoring approaches introduced in the programme evolved over time and informed change at the community level and for programme management. This manuscript describes how Avahan accelerated change through a community mobilisation approach that served the public health imperative of the programme and strengthened the ability, agency and autonomy of communities to bring about more transformative change beyond the programme. Where HIV policy recognises that community mobilisation and linked concepts including structural interventions are desirable to incorporate, the experience of the Avahan programme provides an often called for operational definition of what this is and how it can be undertaken successfully at scale.
Development, public health and participation
Global development approaches have long sought to expand the potential for more effective and equitable outcomes by involving communities to a greater extent in programming. The development discourse around this approach has intensified since the 1990s as concepts of good governance, civil society, participation and community mobilisation have become mainstream.1 ,2 Among the more ubiquitous of the concepts is participation. At its most effective, ‘incorporating participation will mean that processes of policymaking, administration and research become more inclusive, more responsive, more equitable, and so represent more fully the interests of “the people” they claim to serve’.3 Concepts including participation are a central tenet of the World Bank's approaches to poverty reduction and have been consolidated in the Millennium Development Goals and by major donors and academic institutions in the study and pursuit of global health and development.
There has been an evolution in the way participation is conceptualised and used operationally in development settings. It has been challenged as a ‘hurrah’ term that had little meaning or, worse still and paradoxically, as a tool of control to reduce opposition in a project or national process.4 Beyond the more political arguments, participation and linked concepts in the development discourse have been criticised for lacking a framework and tools for analysis.5 Frameworks have since been developed for categorising participation on a relative scale which can allow for better monitoring that categorises a range from weak (instrumental) to strong (transformative) participation.6
A convergence of thought from participatory development, HIV/AIDS and organisational development points to the importance of how implementation is undertaken. The relationships of accountability between governments and civil society, donors and governments or the non-governmental organisations (NGOs) that implement projects and the donor are problematic because they impose limits on the degree to which a project can be changed through a community's involvement. Where communities are empowered they may try to change the way things are done but they are often the least powerful player in a project.7 This change could include aspects of programming or policy which the NGO or donor is committed to but the community feel doesn't serve them. This can cause conflict between communities, implementers, funders and governments, who must take responsibility for grievances, renegotiate different agreements or who may even be drawn into a political confrontation if they listen.8
These dynamics, while recognised in HIV/AIDS programmes, particularly in structural interventions and rights based approaches, have been carefully considered in the field of development, governance and poverty reduction where it has been argued that participation must be monitored just as development outcomes are.8 The field of organisational development applied to NGO management takes this further, offering practical suggestions for managing the grievances, agreements and confrontations that play out in project settings. Sounding more like a business guru truism, NGO management literature talks about being a learning organisation9 or one that can respond to obstacles, even those that are the rules of the game including budgets, policies and staff behaviour.
India and participatory development
India has long been a leader in integrated participatory approaches at a scale rarely possible elsewhere. In the 1970s, with the influence of the Ghandian movement, notable global models were fostered for production cooperatives. Anand Milk Cooperative in Gujarat and sugar cooperatives in Maharashtra proved effective both economically and socially more than 40 years ago.10 The self-help group movement of India is 2.2 million groups strong and has shown a positive impact on empowerment and nutritional uptake in programme areas.11 Other women's groups in India have improved birth outcomes in poor rural communities,10 ,12 as have participatory interventions in other South Asian countries.13
India's effort to foster community development and health is made possible in part by the government's willingness to fund these approaches and work through a massive infrastructure of NGOs with notable, albeit varying, capacity to manage, and a political if not a practical orientation towards empowerment of the marginalised. The disparity between castes, wealth and needs on the ground and the stated ambitions of the Indian government to promote participation and provide information, economic development and health, make it fertile ground for continued contestation of rights and entitlements as well as for the improvement of participatory processes.14
HIV/AIDS and the intersection with social interventions
HIV/AIDS policies and programmes have long been influenced through a sometimes tense, albeit longstanding, relationship with civil society.15 ,16 While community mobilisation and structural interventions are recognised as important, there remains a dearth of data on the relationship between social and HIV outcomes, and a reluctance to describe the operational imperatives, activities and steps that are critical to employ. There is justifiable anxiety that defining the components of community mobilisation or structural interventions will make these prescriptive and they will suffer qualitatively or become irrelevant.17 Introducing effective social interventions in a public health programme may necessitate a commitment to participatory approaches and programme learning which is not without its challenges. Nevertheless, without clear operational guidance or data beyond small-scale programmes, arguments for a sustainable HIV response that addresses the social determinants of HIV/AIDS will not be considered persuasive.18
Avahan, the India AIDS initiative,19 may provide insights into this dilemma.
Avahan was begun in 2003, in the context of a then inadequate collective response to an HIV epidemic that was known to be concentrated, but without sufficient data to precisely characterise the national HIV prevalence rates.20 Subsequently new data, and improved methods and tools have confirmed the concentrated nature of the epidemic and provided more precise estimates of national HIV prevalence, while the national response has scaled up significantly.21–27 Avahan's goal has been to provide comprehensive coverage (as measured by percentage of the denominator accessing services) of a well defined package of services for groups most at risk of acquiring and/or sustaining HIV transmission into the general population. In 2009, at the end of the first phase of the Avahan programme, 320 000 individuals at highest risk (including female sex workers (FSWs), high-risk men who have sex with men (MSM), transgendered people, and injecting drug users (IDUs)) in six high HIV prevalence states in India were receiving a package of HIV prevention intervention services. These include peer-led outreach and education, treatment of sexually transmitted infections (STIs), referrals for HIV and tuberculosis testing and HIV care, free prevention commodities (condoms, and needle/syringe exchange where appropriate) and community mobilisation initiatives to address structural and environmental barriers.28 Funding was provided to seven major state-level implementing partners (‘lead implementing partners’) which sub-contracted to and built the capacity of 116 grassroots Indian NGOs (‘local NGOs’) in 83 districts to implement the programme.29 ‘Community’ in the Avahan programme refers to the high-risk individuals who came together at the more than 500 drop-in centres (DICs) set up by the local NGOs or otherwise created informal (and later formal) groups as part of their interaction with the programme. The efforts of the programme to foster participation and mobilisation of communities through a strategic, evolving approach over a 7-year period is the basis of this case study.
Community mobilisation in Avahan
The concept of community mobilisation in Avahan was influenced by the approach applied by the Sonagachi movement in Kolkata which remains a globally recognised sex worker ‘community’-led structural intervention showing both risk reduction and improvements in social outcomes for sex workers.30 As Avahan undertook implementation in multiple contexts across six Indian states, it became clear that lead implementing partners could not be told to replicate a specific model but needed to have flexibility to design their own strategies for community mobilisation and structural interventions. This they did, allowing for variability in states, districts and sites, shaped in part by the heterogeneous nature of sex work, social and political environments, discrimination and stigma, social entitlement schemes and incentives for community mobilisation.31 The lead implementing partners and the local NGOs were well versed in participatory techniques14 and frequently applied these, resulting in a remarkable degree of innovation and input from communities on the ground. This shaped the programme design in terms of the activities included in community mobilisation and the extent of the monitoring and evaluation effort. The approach was an integrated one where a high degree of participation was built into peer-led outreach, clinical services and commodity distribution. Activities were also fostered in the name of community mobilisation and led by community members, including building access to entitlements, crisis response, advocacy, legal literacy and organisational development of community groups. Among the defining characteristics of the operational approach to roll out community mobilisation were: (i) established but flexible service quality standards; (ii) fostering commitment among leadership from the foundation team, to implementing partners, to NGOs so that the participation of communities was a strong aspiration of the programme; and (iii) flexible and phased implementation of community mobilisation to suit local contexts.
Foundation staff in India worked with lead implementing partners to designate a standard set of activities, the Common Minimum Programme (CMP), for programme-wide implementation.29 The CMP was designed to provide guidance to partners on the standard activities found to be most effective through global and programme experience. Far from being a directive prescription, the CMP integrated innovations from the field and has served as a living document, developed first in 2004 and revised in 2006 and 2010. In practice, decisions on whether to introduce activities into the CMP were made with partners who presented suggestions based on their experience of participatory processes in their programmes. Once activities were included in the CMP it was the responsibility of the lead implementing partners to work with NGOs and communities at the local level to refine strategies and training methods and adjust budgets. Avahan community mobilisation activities are summarised in table 1.
Essential community mobilisation activities in the Avahan Common Minimum Programme (CMP)
Especially from 2006, there was a high degree of focus on community mobilisation from senior Avahan leadership in India, which contributed to the partners' appreciation of its importance. The national management convened semi-annual meetings with senior leadership from the lead implementing partners to discuss programme refinements and best practice; community mobilisation was the central agenda item at the majority of these meetings. The outcome was that community mobilisation approaches across the programme evolved as Avahan learnt what was working and new activities were incorporated or strengthened as the programme evolved.
Across the six states, monitoring of the community mobilisation aspects of the programme was introduced at different times as insight was gained into how to design indicators, tools and processes to be most effective. There is no single baseline for community mobilisation in Avahan as it was not part of the original concept for evaluating the initiative's impact.20 Nevertheless there is now a common approach to evaluation of community mobilization in Avahan, guided by common behavioral surveys implemented across the program, common definitions of variables for analysis and a coordinated effort whereby the practitioners who have been implementing the program for the last seven years are also involved to analyze the data on its effects. This work is captured across this supplement and contributes to the body of learning on the topic, with emerging data to inform the programme and analysis of community mobilisation and outcomes. In practice, tools and methods to measure community mobilisation and associated outcomes were first implemented, then redesigned and repeatedly revised, but the behavioural survey tools use a consistent set of questions asked across all states that offer a focus on community mobilisation and structural interventions. The evolution of the community mobilisation approach of Avahan can be seen as the Avahan programme progressed in Phase 1 and the coordinated evaluation approach was built into Phase 2.19 ,29
Phase 1: working with active, aware, end users of services
Establishing a comprehensive HIV programme in 83 districts across six states was the focus of the programme in Phase 1. Initially, clinic and outreach services were provided in a context where community mobilisation was described in programme documents as the active involvement and ownership of high-risk individuals in all aspects of interventions. At first there was no infrastructure on the ground, and the highly marginalised populations of FSWs, high-risk MSM, transgendered people and IDUs whom the programme sought to serve were not in regular contact with programme staff or services. The lead implementing partners and local NGOs initiated a series of participatory efforts to map and estimate the size of the target populations in order to site and implement accessible and effective services (see table 1).
In the start-up stage of Phase 1, community members, usually peers (ie, paid outreach workers who were members of high-risk communities), were involved in: (i) daily clinic activities related to medical visits and clinic administration, (ii) management of DICs, (iii) regular outreach and education in the community, and (iv) building a supportive environment through community committees, groups and self-help groups.36 ,47
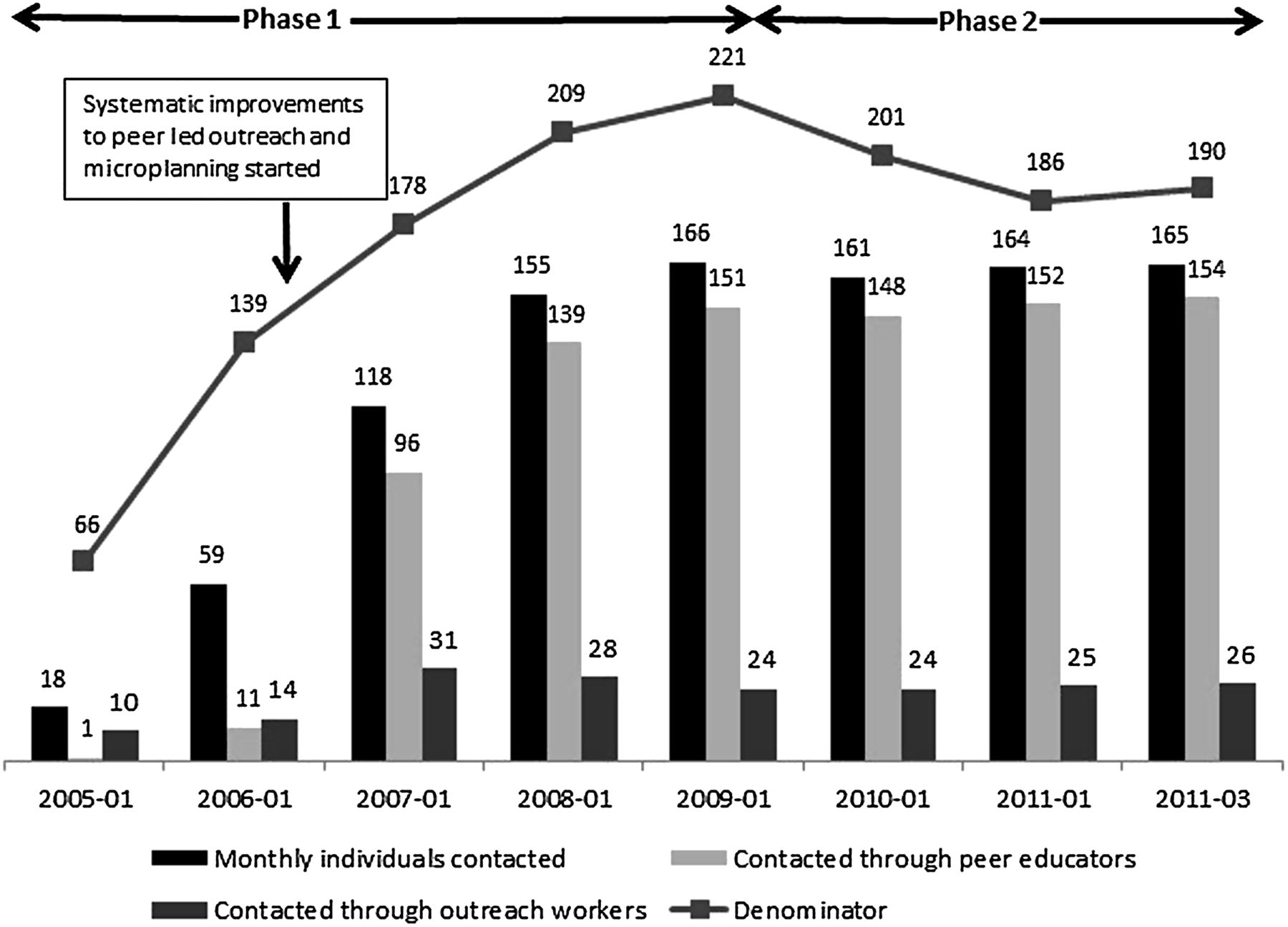
Community mobilisation progressed markedly after the first 2 years of the programme, by which time much of the programme infrastructure had been set up and the focus shifted to improving the quality of outreach, clinics and building access to services. A major catalyst for strengthening community participation was introduced at this time: micro-planning. Micro-planning is a management tool used by peers for recording and analysing individuals' risk and vulnerability in outreach. Peers record data (on a specially designed form that can be understood and completed by those who are not literate) and use it to plan their outreach themselves, based on the individual needs of the population they are serving.36 Among the first encouraging signs that increased participation (albeit in a fairly instrumental way) could improve services was the much more extensive coverage achieved between 2006 and 2007 with the introduction of micro-planning (figure 1). With a more effective system of peer-led outreach, condom distribution improved at a similar rate (figure 3). At the same time, micro-planning allowed peers to build new roles in their communities, new positive identities for sex workers, men who have sex with men, and transgenders that went well beyond condom promotion.

Trends in high-risk individuals contacted monthly by peers versus contacted by outreach workers between January 2005 and March 2011, from Avahan Management Information System (figures are in 1000s).
When peers were more in control of outreach they urged the programme to build in more effective means to address the distal determinants of risk including violence, self-confidence, and debt which they understood to be barriers to condom use and clinical visits.48 Structural interventions, including crisis response, local sensitisation of police, legal literacy and efforts to monitor and more effectively manage community mobilisation were introduced. Crisis response is a community-led system to address incidents of violence, act as a deterrent against future incidents, and tackle longer-term issues of crisis faced by high-risk individuals.49 Associations between violence and HIV outcomes were found after the integration of the crisis response systems.50 Outside the public health argument, addressing crises as part of the programme was part of the effort to mobilise communities, build trust and their collective agency or ability to work together to solve problems.
Practice in the field informed the Avahan approach to interventions: both micro-planning and crisis response were first designed and used by lead implementing partners before being incorporated into the CMP in 2006 and subsequently implemented in all districts. Other activities in this phase of the programme included building access to entitlements such as ration cards and voter IDs. The influence of the participatory approach was not exclusive to peer outreach and community mobilisation activities: STI clinics underwent a progressive approach to engaging communities, whose involvement in managing the clinics progressed markedly between 2005 and 2008.41 During the same period the rates of STI syndromes went down while health-seeking behaviour, measured by STI clinic visits by MSM, FSWs and IDUs increased markedly51 (figure 2).
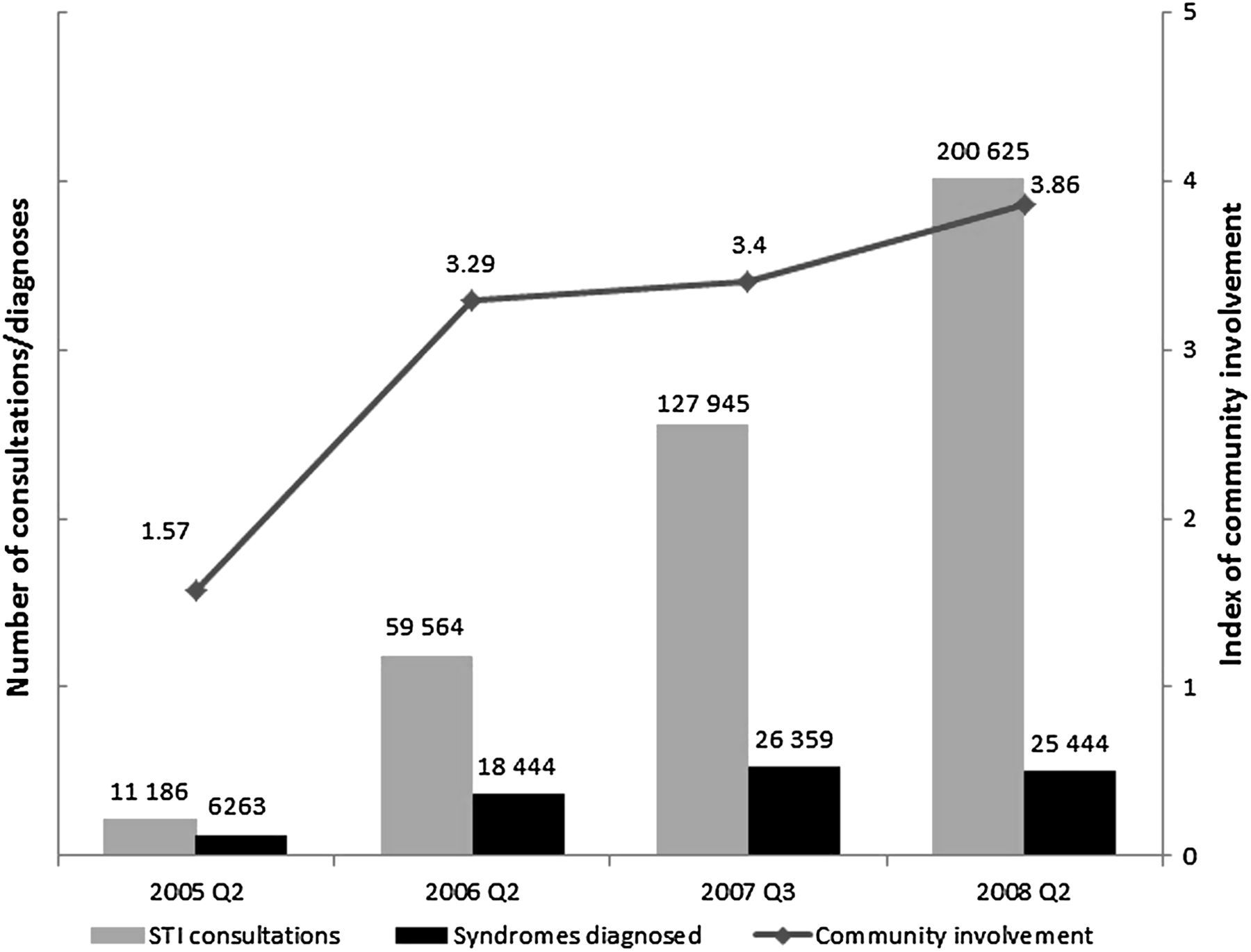
Trends in high-risk individuals attending Avahan-supported clinics for sexually transmitted infection (STI) visits (symptoms or check-up); having an STI syndrome diagnosed is charted against an externally determined index of community involvement in the clinic. Adapted from Jana et al30 and Halli et al.31

Trends in percentage of high-risk individuals contacted by peer educators and number of condoms distributed by non-governmental organisations from Avahan routine monitoring information system. Available only for Avahan Phase 1.
In 2007, monthly monitoring for community mobilisation and a management tool called the diagnostic were introduced. The logic model for community mobilisation in Avahan was not detailed enough to inform these tools, and this, coupled with the challenge of designing routine quantitative indicators to inform qualitative processes, meant that both efforts were modified extensively over the subsequent 2 years until they were eventually integrated into new monitoring tools in Phase 2 of Avahan. The new form of these tools can be seen in the community ownership and preparedness index (COPI) and behavioural tracking surveys complementing the revised logic model.45 ,52
Among the routine programme indicators that were problematic to collect through routine monthly monitoring were the number of community-based organisations and number of incidents of violence. Once the community-based organisations indicator was integrated into the reporting system, the number of reported groups increased much more rapidly than expected, and partners provided feedback that the indicator was driving processes away from genuine mobilisation and towards registering groups that were not actually functional, in order to meet perceived targets. The violence indicator was problematic because definitions of violence were not normalised in crisis response systems and data often went unreported when incidents were resolved quickly. In retrospect the social desirability bias that characterises measurement of these indicators warranted a more invested monitoring activity to define the qualitative aspects of the indicators and more intensive programme work to address these.
Early attempts to measure the relationship between community changes through mobilisation and outcomes were similarly problematic. Among the limited indicators placed in the Integrated Biological and Behavioural Assessment, Round 143 was: Are you a member of a community group? Analysis by the World Bank on the association between self-help group membership in India and empowerment found that empowerment increased among all women in programme areas irrespective of their participation in self-help groups, suggesting positive externalities.11 Ethnographic research supported in the Avahan programme under the Parivartan project similarly found that membership alone could not define the experience of community mobilisation, but that community-level changes needed to be understood by more mediating psycho-social factors.53 A behavioural tracking survey, based on a cross-sectional behavioural survey implemented through the Parivartan project, was introduced in 2009, a monitoring tool to be implemented in two rounds in all six programme states. Indicator sets to understand community-level changes have constructs for individual agency, confidence, collective agency, social cohesion and other areas with conceptual underpinnings from sociology and behavioural science to understand the functional changes within the community as a result of community mobilisation. This has proved to be more useful for understanding how community mobilisation may lead to improved health outcomes, as described in publications elsewhere (table 3).
After 61 months, at the end of Phase 1, the programme had reached most of its targets for infrastructure and service delivery, establishing 1897 clinics and 558 DICs, and reaching 93% of the monthly outreach coverage, 81% of the clinic attendance and 100% of the condom distribution targets.20 More relevant to community mobilisation were the increases in service coverage and health-seeking behaviour that seemed to be related to efforts to engage communities more in improving clinics and in outreach through micro-planning.
Phase 2: programme transition
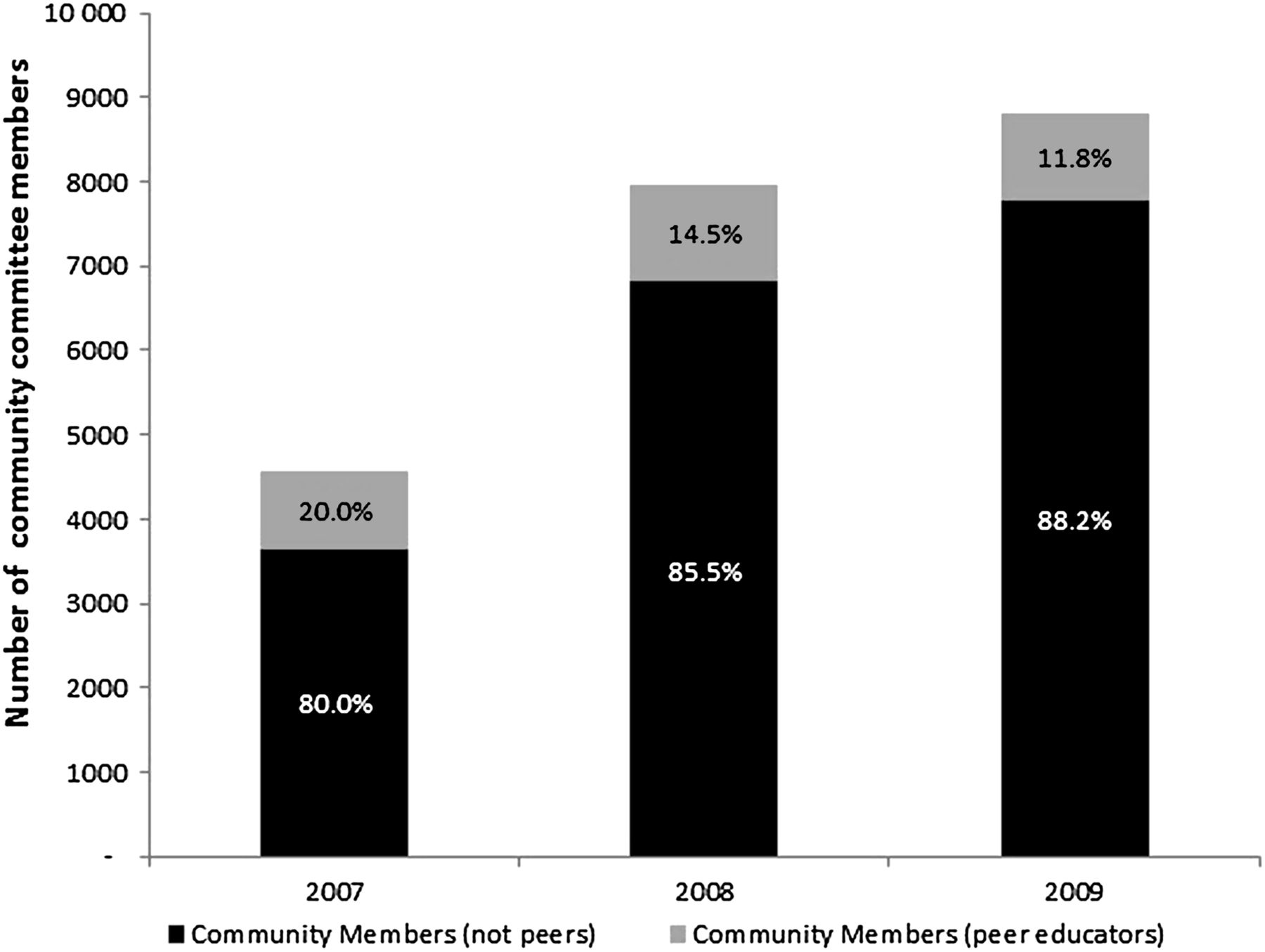
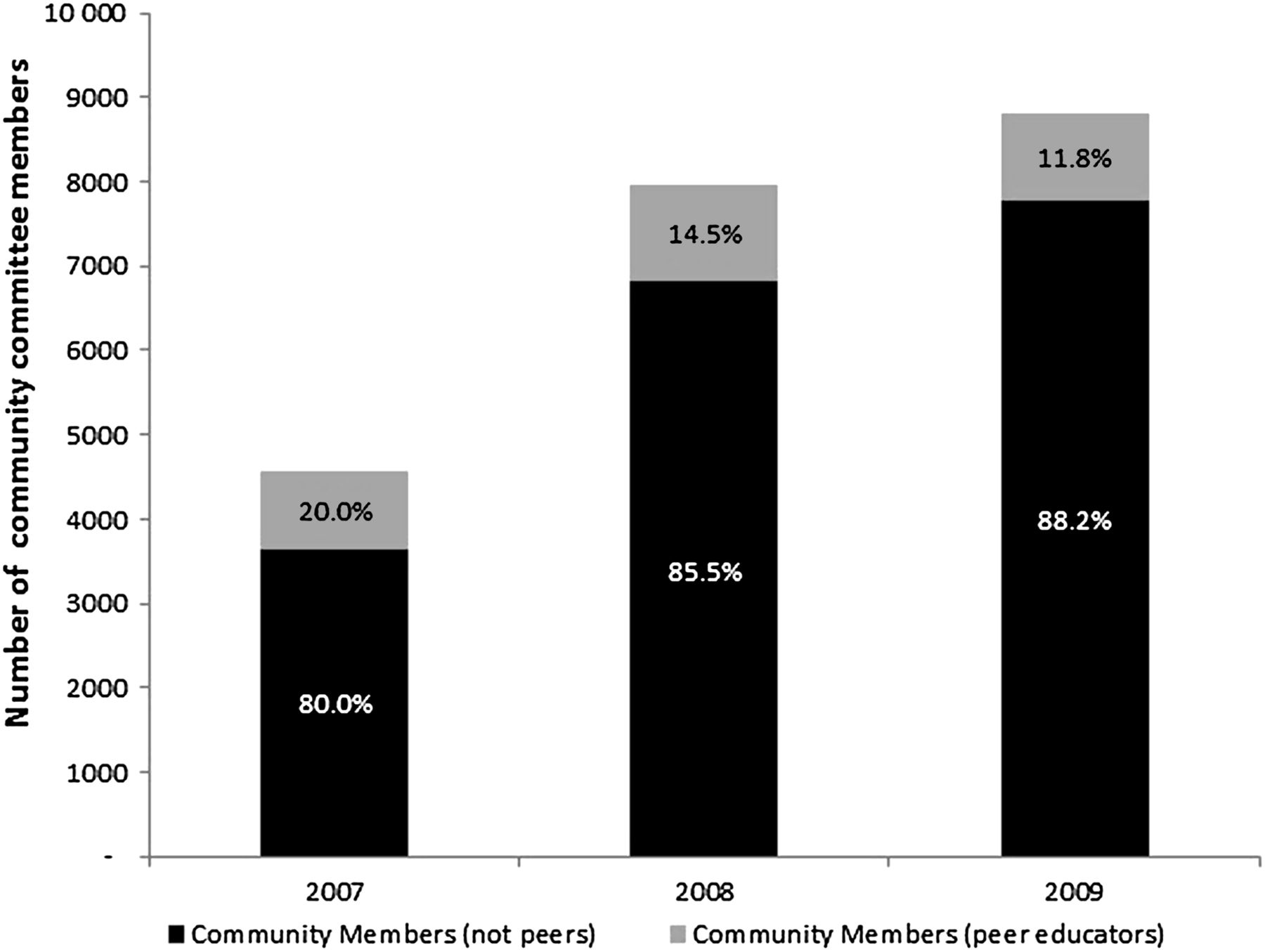
This phase of Avahan, still underway at the time of writing, focuses on the programme shifts required for the Avahan service package to be integrated with the government of India's National AIDS Control Programme in preparation for the end of Avahan funding in 2013. There is also a focus on preparing community-based groups to lead some components of the programme. Service oversight committees were introduced in Phase 1 and as Phase 2 progressed, they became increasingly led by community non-peers to ensure that a sustainable social accountability function was established between service providers and communities (figure 4). In large measure this accountability function should be integrated into the work of community based organisations and funded independently. Two critical milestones were recognised as important for the community mobilisation transition objective of Avahan: (i) community groups must be strengthened organisationally, and (ii) community action for vulnerability reduction (ie, activities addressing violence and economic security) and advocacy must be fostered.60
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Membership and percentage of Avahan community committees with non-peer community members versus peer-educator community members making up committees over time, from Avahan routine monitoring information system. Available only for Avahan Phase 1.
In the transition, partners have focused on strengthening leadership in community organisations, processes of governance, management of activities, and linking the community organisations to larger networks of community groups, particularly at the state level where policy and budgetary decisions are made for HIV/AIDS and social programmes. From a participation standpoint these efforts work to build a more transformative role for communities although much remains to be done.
Discussion
The Avahan experience may provide insights into how to scale and manage a community mobilisation approach in an HIV/AIDS prevention programme. Specific activities including micro-planning, structural interventions including crisis response and community organisational development were built in phases with operational learning (table 1). While it was a challenge to determine how to measure qualitative factors of community mobilisation, it proved essential to informing both the programme and evaluation (table 2). The early evidence coming out of the programme addresses HIV prevention explicitly, structural factors and organisational development supporting the argument that the strength of community participation in the programme and extent of community level changes, including collective agency, build the effectiveness of risk reduction (table 3). Measurement of these factors may prove relevant to build on in further research. Similarly, where the self-reporting monitoring of violence and community group activities faced subjectivity and problematic reporting it may be instructive to other programmes that more rigorous efforts must be undertaken to effectively address these factors. Emerging evidence which shows the effect of stronger participation and violence addressal on HIV outcomes should justify a more reliable evaluation effort of these interventions.
Monitoring, evaluation and knowledge building efforts to document community mobilisation in Avahan
Avahan community mobilisation and structural intervention data published to date
The utility and ethics of employing participatory monitoring and planning through the COPI46 ,60 is addressed at length elsewhere and is considered to be among the most important management techniques for scaling community mobilisation as it provided both monitoring data to track change and anchored processes to precipitate change. The COPI addresses some of the more challenging dynamics of participatory processes and seeks to gauge, among other things, the level of autonomous decision-making and planning undertaken by communities beyond peer involvement, so that the programme can respond with activities to support further evolution.60
The Avahan community mobilisation management approach led to necessary programmatic, budgetary and organisational change in order to respond to and facilitate transformative participation in communities.9 Avahan's changing CMP, was informed by approaches for managing organisational dynamics and planning with communities that led to better informed programs or better understanding of useful measures for community mobilization in our setting. Avahan's common approach to monitoring and evaluation attempts to build a body of results that better illustrate the changes occurring in the program and how community mobilization, behavior change and HIV outcomes interact. It may be worth considering therefore that complex public health responses are best managed and measured through two constantly shifting lenses - one that seeks to understand as closely as possible an individual's experiences of distal and proximate risks and the other which seeks to extrapolate and change policy, budgets and staff orientation to address these individual's needs.
The phasing of community mobilisation was undertaken as a necessity for managing a scaled programme in response to a public health imperative to prevent HIV among the population by the most effective, efficient and fundamentally ethical means.61 In the first 2 years of the programme, community mobilisation was approached in a fairly instrumental way, particularly in the role played by paid peers. They were told how and what to do in their outreach, with little autonomy until the introduction of micro-planning. Peers then were not restricted to activities ordained by the local NGO-driven project: they prioritised and managed outreach fairly independently, argued for the introduction of programme activities including crisis response, and led the planning and implementation for it. Managing for this change requires deliberate action to promote community agendas within the programme and create space for communities to shape services and budgets, and redefine programme priorities. If the role of the community is limited to programme implementation, with incentives of payment and programme association alone, the transformative potential of the community's participation will be limited and the numbers of individuals potentially affected will be limited to the number of peers in the programme. Indeed, these issues have been confronted in similar settings, and it has been argued that operational contexts in public health settings cannot avoid them but it may be possible to better respond.
What is already known on this subject
This case study aims to complement debates about participation, organisational development and scaling up community mobilisation with an operational example of an HIV prevention programme.
While community mobilisation approaches and structural interventions have been carefully explored, learning is typically restricted to projects that cover at most several thousand individuals, and replication and managing for scale are rarely considered.
This case study examines a number of challenges that are central to current debates: the challenge of supporting transformative change for communities versus focusing on the most efficient means to reduce risk; fostering community- led processes versus designing standards that can be followed across a scaled programme; and applying measurement to understand qualitative differences on the ground, often considered context-dependent.
What this study adds
The Avahan experience with community mobilisation allows us to explore how a large-scale public health intervention using a community mobilisation approach navigated these tensions and addressed them.
Among the topics reflected on from 7 years of learning are how a scaled programme can facilitate meaningful participatory processes, incorporate effective monitoring and respond to change through flexible management.
It advocates for managing a phased community mobilisation approach whereby the initial emphasis may be the programme working for the community, before it is really operated with the community and finally becomes an effort led by the community.
Although it remains inconclusive, written while the programme is still operating, it offers lessons from commonly experienced challenges and insights into designing a measurement approach, and provides a synthesis of community mobilisation programme data to date from Avahan.
Acknowledgments
We wish to acknowledge the efforts of Avahan state level and community mobilisation partners whose efforts are described here and without whom these lessons would not have been learnt. Avahan's lead implementing and data collection partners include: Alliance for AIDS Action Project (India HIV/AIDS Alliance, Andhra Pradesh), Swagati and Nestam Projects (Hindustan Latex Family Planning Promotion Trust, Andhra Pradesh), Corridors and Project Sankalp (Karnataka Health Promotion Trust, Karnataka), Aastha Project (Family Health International, Maharashtra), Mukta Project (Pathfinder International, Maharashtra), Project ORCHID (Emmanuel Hospital Association, Manipur and Nagaland) and Tamil Nadu AIDS Initiative (Voluntary Health Services, Tamil Nadu). We acknowledge James Baer for his editorial work.
References
Footnotes
Linked articles 200562, 200487, 200465, 200475, 200514, 200511, 200832, 201065, 200478, 200508, 200590.
Funding This work was supported by the Bill & Melinda Gates Foundation under the HIV/AIDS Division through a range of grants in the Avahan portfolio, including grants of the following identification numbers: 29868, 29928, 30080, 30111, 30121, 30138, 30148, 30177, 30183, 30553, 31280 39418, and 5189.
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement An open access data policy is in place for all data associated with the project.
Linked Articles
- Research report
- Research report
- Research report
- Research report
- Research report
- Research report
- Research report
- Research report
- Research report
- Research report
- Research report