Article Text

Abstract
Objective: The objective of the present study was to examine if the change in the suicide rate is associated with individuals’ use of antidepressants as has been suggested by ecological studies.
Design: Decomposition of suicide rates by antidepressant treatment group.
Setting: Population-based record linkage.
Participants: All individuals aged 50 years and older living in Denmark between 1 January 1996 and 31 December 2000 (N = 2 100 808).
Main outcome measures: Suicide rates are calculated according to current antidepressant treatment status (no treatment, tricyclic antidepressants (TCA), selective serotonin reuptake inhibitors (SSRI), other antidepressants). The change in the suicide rate during 1996–2000 was decomposed by treatment group.
Results: Only one in five older adults dying by suicide was in treatment at the time of death. Whereas the male suicide rate declined by 9.7 suicides per 100 000, recipients of antidepressants contributed to the decline by 0.9 suicides. Women redeeming antidepressant prescriptions accounted for 0.4 suicides of the observed reduction of 3.3 per 100 000. The average suicide rates for men receiving TCA and SSRI were 153.3 and 169.0 per 100 000 person-years, respectively. Among older women, both TCA and SSRI users had an average suicide rate of 68.8 per 100 000 over the period examined.
Conclusions: Just a small proportion of older adults dying by suicide were found to be in treatment with antidepressants at the time of death. Individuals in active treatment with antidepressants seem to account for 10% of the decline in the suicide rate. Nevertheless, suicides might be prevented by more effective treatment.
Statistics from Altmetric.com
Suicide is a major health problem in many countries. Despite national prevention programmes aimed at reducing the number,1 it is estimated that 815 000 individuals die by suicide each year worldwide.2
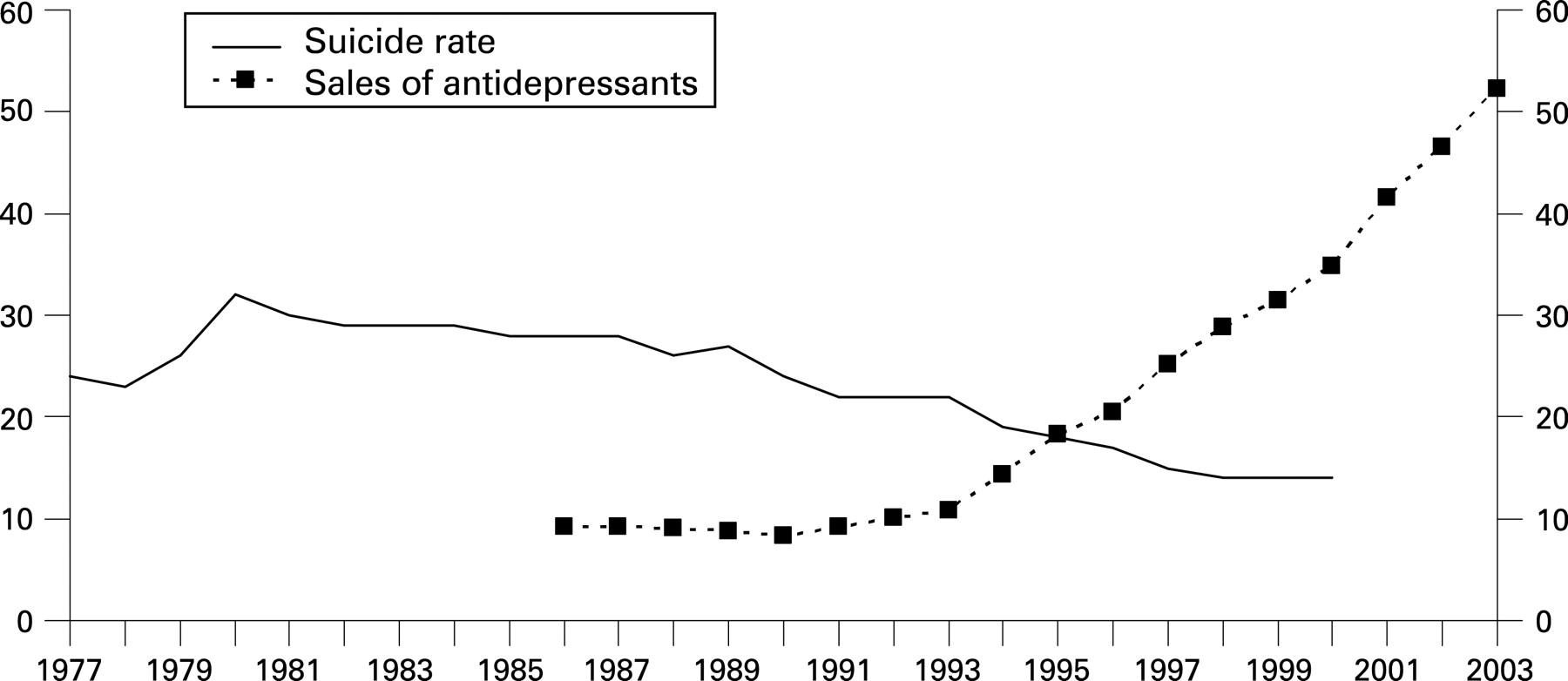
In many industrialised countries suicide rates have decreased in recent years, a phenomenon that has been related to the increased sales of antidepressants, in particular selective serotonin reuptake inhibitors (SSRI).3–16 Others have found no such association.17–19 Ecological studies have assessed the association by correlating the rate of dispensed antidepressants (measured as use per capita) with the trend in the overall suicide rate,3–5 8 11 13 16 18 19 or used extrapolated sample data.6 7 9 10 12 14 17
Meta-analyses of randomised clinical trials have not found an effect on the risk of suicide among SSRI recipients.20 21 It has, however, been estimated that a fivefold increase in the use of antidepressants may result in a 25% decline in the suicide rate and that SSRI may have saved as many as 33 600 lives in the United States since their introduction.13 14 Nevertheless, the exact contribution by individuals exposed to antidepressants to the change in the suicide rate remains to be assessed.9 10 13 Danish register data offer the opportunity to analyse individual-level data for an entire nation through linkage via a unique personal identifier.22
Sales of antidepressants have increased markedly from 8.4 in 1990 to 52.2 in 2000 per 1000 inhabitants in Denmark (see fig 1).23–26 Older adults are receiving antidepressants at higher rates than younger age groups.27 Furthermore, older adults are accountable for the highest suicide rates in Denmark. The suicide rate among individuals aged 50 years and over declined from 52.2 to 22.1 per 100 000 during 1980 to 2000.28–30 If an association between antidepressants and the overall suicide rate exists, it may thus be most apparent among individuals in the second half of life.13
Using decomposition techniques, it is possible to calculate the impact of antidepressant recipients on the change in the suicide rate. The purpose of the current study was to determine whether individuals redeeming antidepressants, in particular SSRI, contributed to the decline in the overall suicide rate among individuals aged 50 years and over.
METHODS
Register data
Data covering the entire population aged 50 years and older living in Denmark during the period 1 January 1996 to 31 December 2000 were obtained from the Centralised Civil Register, the Registry of Causes of Death and the Register of Medical Product Statistics.22 The latter register contains information on all individuals filling antidepressant prescriptions at pharmacies. Using the unique personal identifier, nationwide data were linked on an individual level by Statistics Denmark. Permissions for data linkage were obtained from the Danish Medicines Agency, the Danish Data Protection Agency and the University of Rochester Research Subjects Review Board. As the analysis is based on existing data, informed consent from subjects was not required.
The different types of antidepressants were classified by their anatomical chemical therapeutic group as tricyclic antidepressants (TCA; amitriptyline, amoxapine, clomipramine, dosulepin, doxepin, imipramine, imipramine oxide, lofepramine, maprotiline, nortriptyline, opipramol, protriptyline, trimipramine), SSRI (citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline) and other antidepressants (isocarboxazid, mianserin, mirtazapine, moclobemide, nefazodone, reboxetine). The group of other antidepressants also includes individuals who were currently receiving two or more different types of antidepressants.
A relatively large proportion of individuals who receive antidepressants discontinue their medication during the first prescription period, ie, they never redeem a second prescription.27 31 Therefore, subjects were considered as being in treatment with an antidepressant from the date that they filled their second prescription at a pharmacy. This approach also helped to ensure that the duration of exposure was sufficient to have a beneficial effect. The treatment period was registered as being discontinued when the receipient did not hand in a new prescription within a given timeframe based on the number of pills dispensed. Comparable assumptions have been applied in previous studies using the same data source.27 Prescriptions redeemed during 1995 were assessed to determine which individuals were considered to be in treatment at 1 January 1996.
The subjects filled a total of 3 722 166 prescriptions during the observation period, of which 583 149 were first prescriptions. In all, 19 313 individuals either died or migrated before the date when the second prescription was expected to be filled. Among the remaining group, 299 440 individuals (53%) handed in a second prescription and, therefore, were considered as being in treatment. There was little variation in the discontinuation rate with regard to drug type. These figures are analogous to previous reports.27
During the five-year observation period, individuals migrating or dying by causes other than suicide were censored at the date of the event. Suicide was defined as “X60–X84: Intentional self-harm” and “Y87: Sequelae of intentional self-harm, assault and events of undetermined intent” according to the 10th revision of the International Classification of Diseases.32
Decomposition method
Decomposition techniques, as used in demographic studies,33 were applied to calculate the exact contribution by each treatment group to the change in the overall suicide rate. The treatment-specific suicide rate for the whole population aged 50 years and over in year t, Si(t), is defined as Si(t) = Di(t)/Pi(t), where Di(t) and Pi(t) denote the number of deaths by suicide and the person-years lived for treatment group i in year t, respectively.
The overall suicide rate is equal to the sum of each treatment group’s suicide rate multiplied by the proportion of person-years spent in that group at time t. Let the population composition by treatment group be denoted by Ci(t) = Pi(t)/P(t), the suicide rate in year t is then

The change in the suicide rate is obtained by calculating the derivative with respect to the time of equation 1

As shown in equation 2, the precise contribution by each treatment group i to the overall change is decomposed into two components. The first component covers changes in the overall suicide rate caused by changes in the treatment-specific suicide rate and the second component accounts for changes in the population composition. The sum of the two components provides the treatment group i’s total contribution to the change in the overall suicide rate.
To approximate derivatives we assumed that all variables follow linear trends as used in standard applications of decomposition techniques.33 34 As our study includes the entire Danish population aged 50 years and older, the use of statistical inference and hypothesis testing is not required for sample generalisation.35 Standard deviations were calculated based on the ratio of the treatment-specific suicide rates divided by their population size.36
RESULTS
In all, 2 100 808 individuals (982 217 men and 1 118 591 women) accounting for 8 805 892 person-years (4 065 852 men, 4 740 040 women) were included in the analysis. During the five-year observation period, a total of 2136 individuals (1426 men and 710 women) died by suicide. Of those, 501 (35%) men and 398 (56%) women had received one or more antidepressant medication within their last year, as shown in table 1. Approximately 17% of men and 28% of women had redeemed antidepressants within the last month of life. These figures are based on first as well as later prescriptions within a treatment sequence.
The average suicide rate over the years examined for older men receiving TCA was 153.3 per 100 000 person-years, whereas the rate for SSRI was 169.0 and other types of antidepressants 273.2. The rate for men not in treatment was 30.7 per 100 000. For women, the average suicide rates for TCA, SSRI and other types of antidepressants were 68.8, 68.8 and 112.6 per 100 000, respectively, whereas those not in treatment had a suicide rate of 11.0. The treatment-specific suicide rates by calendar year are displayed in fig 2.

{kind=link}
{kind=link}
During the five-year observation period, the percentage of person-years spent in antidepressant treatment increased steadily from 2.4% in 1996 to 3.3% in 2000 for men and from 5.3% to 7.0% for women aged 50 years and over (table 2). Approximately 14% of men and 30% of women who died by suicide were considered to be in treatment with antidepressants at the time of death. The overall suicide rate for men aged 50 years and over decreased from 41.8 in 1996 to 32.1 per 100 000 in 2000, a change of 9.7 suicides per 100 000. The female rate declined by 3.7 suicides per 100 000 from 16.7 to 13.0 per 100 000 over the same period.
Table 3 lists the results of the decomposition analysis for men and for women. The total contribution by each treatment group to the change in the overall suicide rate is shown in the last column. Men and women who were not in treatment accounted for the major share of the decline in the suicide rate—reductions of 8.72 and 3.3 suicides per 100 000, respectively. Men receiving antidepressants accounted for a decline in the rate of 0.94 suicides per 100 000, whereas the female treatment groups contributed with 0.40 suicides per 100 000. With regard to specific types of antidepressants, users of TCA contributed to, whereas those prescribed other types of antidepressants opposed, the decline in the suicide rate. Although male users of SSRI contributed to the decline, women in SSRI treatment opposed the decline.
What is already known on this subject
Decreasing suicide rates have been observed across many countries. Ecological studies have correlated this decline with increasing sales of antidepressants.
The total contribution of each treatment group to the change in the suicide rate is equal to the sum of the two components, change in the treatment-specific suicide rate and change in the population composition. As seen in the first column of table 3, all groups receiving antidepressants contributed to the decline in terms of their suicide rate (changes in treatment-specific suicide rate). Nevertheless, the second column (changes in the population composition) lists large increases in the number of people receiving SSRI and other types of antidepressants. The second component thus counteracted the first component.
A sensitivity analysis using a different definition for active treatment was carried out (see supplementary tables A1 and A2 available online only). When considering subjects as being in treatment with antidepressants from the date of the first prescription, approximately 25% of male and 40% of female suicides occurred during treatment. Men in treatment with antidepressants then contributed with 0.82 to the decline of 9.66 suicides per 100 000. Women in treatment contributed with 0.68 to the decline of 3.70 suicides per 100 000.
What this study adds
This is, to our knowledge, is the first study to decompose the contribution by antidepressants to the change in the suicide rate by using individual-level data. Our findings show that the decrease in the suicide rate seems to be the result of other factors.
Policy implications
Suicide prevention strategies cannot rely on the increased use of antidepressants as a sole resource for obtaining reductions in the number of suicides
More effective identification of affective disorders in older adults is needed. Just a small proportion of those dying by suicide were found to be in active treatment with antidepressants
Future research is needed to determine which other factors contributed to the decline in the suicide rate in Denmark and elsewhere
DISCUSSION
This is to our knowledge the first study to calculate nationwide suicide rates for individuals in treatment with antidepressant medications. Whereas individuals in treatment with TCA and SSRI had suicide rates of approximately the same level, other types of antidepressants were above these. Our findings indicate that only a small proportion of adults over the age of 50 years who died by suicide had recently redeemed prescriptions for antidepressants. It was found, using individual-level data, that treatment with antidepressants made a contribution to the decline in the overall suicide rate during the study period. The major share, however, seems to be explained through other components.
Change in overall suicide rate
We observed a decline in the overall suicide rate at a time when the rate of redeemed antidepressants increased. This corresponds to the findings of most previous studies.3–11 13–16 By decomposing the change in the suicide rate, we found that individuals receiving antidepressants do contribute to the decline in the overall suicide rate. Nonetheless, the major share is accounted for by individuals not in active treatment with antidepressants.
Given the large reductions in the treatment-specific suicide rates, it may at first seem surprising that individuals in active treatment with antidepressants do not contribute more to the decline in the overall suicide rate. The large number of individuals transferred from the “no antidepressant” group to the “SSRI” and “other types” treatment groups, which have higher suicide rates, oppose the decline in the treatment-specific suicide rates. This is seen in the changes in the population composition in the second column of table 3.
We used a rigorous definition in order to limit the subjects to those in active ongoing treatment. Future studies might benefit from examining the impact among past users of antidepressants. Given the wide spectrum of symptoms for which SSRI are administered, however, from major to subsyndromal depression, pain syndromes, irritable bowel syndrome and sexual dysfunction,37–39 it would also be important to assess the diagnoses for which the medicine was prescribed.
Suicide among antidepressant users
The rates of suicide among individuals receiving TCA and SSRI were approximately five to six times higher than among individuals who were not in treatment. The category of other types of antidepressants also includes individuals receiving combined drug treatments. The higher suicide rate of individuals in this group might thus reflect more complex or treatment-resistant disorders. Nationwide suicide rates for individuals in treatment with antidepressants have not previously been published and only few reports of sample-based suicide rates exist. Meta-analyses of randomised clinical trials list suicide rates of 500–590 per 100 000 for SSRI and 448–760 per 100 000 for TCA and other antidepressants.40 41 These rates are substantially higher than the findings from the current study, perhaps because they represent a select patient group with a higher suicide risk. A Danish study estimating suicide rates for different antidepressant types also found levels higher than those reported here, the study included subjects aged 18 years and over, which might explain the divergence in findings.42 Apart from the first 30 days of treatment, Canadian findings suggest that the suicide risk does not differ substantially with respect to the type of antidepressants.43 Our findings partly support this observation.
In all, 20% of the individuals who died by suicide had redeemed a prescription for antidepressants within their last month of life; 37% in the last six months. A regional Danish study found that one quarter of all suicides were considered to be in treatment with antidepressants one month before death.44 Another study, however, found a larger proportion had received antidepressants within the calendar year of the suicide.42 In comparison, Swedish and Canadian findings report that 48% and 32% of suicides, respectively, in an elderly sample had received antidepressants within the last six months.43 45 Our findings, which are based on the entire nation of adults aged 50 years or older, are comparable to these reports.
Clinically, it is highly relevant that only a small proportion, one in five, were at the time of death considered as being in treatment. This observation is supported by forensic data showing that 20% of examined suicides of a wider age range had traces of antidepressants in postmortem toxicology.46 It is estimated that more than 70% of older adults who die by suicide suffer from mood disorders.47 Given that antidepressants are the most commonly applied therapy for mood disorders, our findings suggest that a strikingly large proportion of the older adults dying by suicide are not receiving the treatment indicated.
Limitations
Limitations of the study must be acknowledged. First, the findings could be influenced by the definitions regarding length of treatment. Additional sensitivity analysis in which subjects were considered as being in treatment from the first prescription onwards provided comparable results to those shown here (see supplementary tables A1 and A2 available online only). Second, it is unknown whether the subjects who were administered antidepressants actually consumed the drug. Nevertheless, by only including individuals who redeemed a second prescription, we increased the likelihood that subjects were compliant with treatment and that they received doses of sufficient duration to derive therapeutic benefit. Third, we have no information regarding the distribution of free samples of antidepressants by general practitioners or during hospital admissions, other non-pharmacological therapies, diagnosis or severity of the treated disorder. Although it would have been informative to know the diagnoses, our objective of examining whether those receiving antidepressants contributed to the decline in the overall suicide rate remains unaffected by this shortcoming.
Specific subpopulations, such as individuals with mood disorders who are not receiving antidepressants, might experience a higher suicide rate than individuals receiving antidepressants. One could speculate that the suicide rate of this subpopulation would be affected if the proportion using antidepressants increased. As there is no indicator in the data on individuals experiencing mood disorders but not receiving treatment, it is beyond the scope of the present study to examine this hypothesis. Furthermore, we are assuming that the population segment in treatment with antidepressants in 1996 was comparable to those in treatment in 2000.
In conclusion, it was found that only a small proportion, one in five, was considered to be in treatment with antidepressants when dying by suicide. We found that, when examining the association on an individual level, people in treatment with antidepressants during 1996–2000 contributed with 10% to the decline in the suicide rate of adults aged 50 years and over. The major share of the decline occurred among individuals not in active treatment. More aggressive treatment of individuals with affective illness is indicated. At the same time, substantial reductions in suicide rates at the population level may hinge on the development of universal and selective preventive strategies that target larger population segments.48 Future research may profit from examining the influence of societal factors on changes in the suicide rate using individual-level data.
Acknowledgments
The authors wish to thank Dr Dorte G. Hansen from the University of Southern Denmark for input on assumptions regarding compliance with treatment. Comments on an earlier draft of the manuscript were obtained from: Dr Robert Schoen, Population Research Institute, Pennsylvania State University; Dr Kenneth Conner, Dr Kerry Knox as well as the Study Group on Suicide in Older Adults, University of Rochester Medical Center; Esben Agerbo and colleagues from the National Centre of Register-based Research, University of Aarhus.
REFERENCES
Supplementary materials
web only appendix 62/5/448
Files in this Data Supplement:
Footnotes
Funding: Funding for the current project was provided by the Danish Velux Foundation, American Foundation for Suicide Prevention, and National Institute of Aging (grant R01AG11552). Psychiatric epidemiological research at the National Centre for Register-based Research is partly funded through a collaborative agreement with Centre for Basic Psychiatric Research, Psychiatric Hospital in Aarhus, Denmark.
Competing interests: None.
Linked Articles
- In this issue