Article Text

Abstract
Background Studies have shown that malnutrition in early life has a negative effect on midlife cognitive functions. Little is known, however, about the relationship between early-life malnutrition and visual, hearing or dual sensory impairments in adulthood. This study aims to investigate the association between exposure to the 1959–1961 Chinese famine in early life and sensory impairments in adulthood.
Methods A total of 6347 adults born between 1952 and 1964 surveyed in the 2015 China Health and Retirement Longitudinal Study were included in this study. The presence of sensory impairments was identified by self-reported assessment of visual and hearing functions. The associations between multi-stage early-life famine exposure and sensory functions were estimated using the multiple generalised linear model.
Results Compared with the unexposed group, respondents exposed to famine in the fetal period and late childhood had a significantly higher risk of hearing impairment (OR 1.54, 95% CI 1.06 to 2.24; OR 1.75, 95% CI 1.23 to 2.50) and dual sensory impairments (OR 1.45, 95% CI 1.00 to 2.11; OR 1.55, 95% CI 1.09 to 2.21), respectively. Furthermore, in severely famine-affected areas, the early, mid and late childhood-exposed groups were more likely to have hearing and dual sensory impairments than the unexposed group. Those associations were not observed in less famine-affected areas. However, no significant association was found between famine exposure and visual impairment in early-life famine-exposed group.
Conclusion Exposure to Chinese famine in the fetal period and late childhood was linked to hearing and dual sensory impairments in adulthood.
- Fetal
- lifecourse/ childhood circumstances
- nutrition
Statistics from Altmetric.com
INTRODUCTION
Visual, hearing and dual sensory impairments are common among older adults1 and have been consistently associated with greater risk of cognitive decline, depression symptoms and reduction in quality of life.2 3 Intrauterine nutrition may play an important role in the development of sensory systems. For instance, a cross-sectional observational study that sampled 433 390 individuals in the UK suggests that being underweight at birth is a risk factor for poorer vision, hearing and cognition in midlife.4 As a major health problem, malnutrition affects millions of children across the world, especially in low- and middle-income countries.5
Historical famines provide a unique opportunity to study the long-term association between nutritional deprivation in early life and age-related visual and hearing impairments. As one of the largest catastrophic events in recent human history, the 1959–1961 Chinese famine caused approximately 30 million excess deaths.6 In contrast to the 1944–1945 Dutch famine and 1932–1933 Holodomor famine, Chinese famine lasted for 3 years and influenced almost every region of China.6 The 1959–1961 Chinese famine allows researchers to investigate the long-term influence of malnutrition in intrauterine and childhood periods among the non-European population.
A previous study has found that pregnancy and infancy malnutrition played an important role in later disease susceptibility.7 Deficits in sensory functions like vision and hearing impairments may be a risk factor for the development of Alzheimer’s disease (AD) and other late-life degenerative conditions.8 However, the association between severe nutritional deficiency during early life and sensory impairments remains to be investigated. Thus, it is salient to examine the associations between severe nutritional deprivation during early life and visual, hearing, and dual sensory impairments (visual and hearing) in adulthood. In this study, we used data from the 2015 China Health and Retirement Longitudinal Study (CHARLS) to examine this topic.
METHODS
Study population
Data from the 2015 CHARLS were used to investigate the association between fetal/childhood famine exposure and adult sensory functions. CHARLS is an ongoing national longitudinal study of Chinese adults aged 45 years and older, which collects an excellent nationwide sample to represent the middle-aged and elderly in China. Its rationale and cohort design has previously been described in detail.9 The 2015 wave is the latest follow-up survey, which sampled 21 095 respondents, and all of them signed informed consent. The programme protocol was in line with the Declaration of Helsinki and was ethically approved by the Biomedical Ethics Review Committee of Peking University (approval number: IRB00001052–11 015).10
Famine cohorts and area categories
Figure 1 shows the schematic flow of sample selection. A total of 6347 samples were finally included based on the following inclusion and exclusion criteria. Inclusion criteria were as follows: born between 1952 and 1964; having the ability to communicate and recall clearly. Exclusion criteria were as follows: legally blind; suffering from severe memory-related diseases (such as AD, brain atrophy, Parkinson’s disease); having missing values of physical examination and sensory measures. In line with previous studies on Chinese famine, respondents were categorised into five groups based on their date of birth: the unexposed group (1 October 1962–30 September 1964), the fetal-exposed group (1 October 1959–30 September 1961), the early childhood-exposed group (1 October 1956–30 September 1958), the mid childhood-exposed group (1 October 1954–30 September 1956) and the late childhood-exposed group (1 October 1952–30 September 1954).
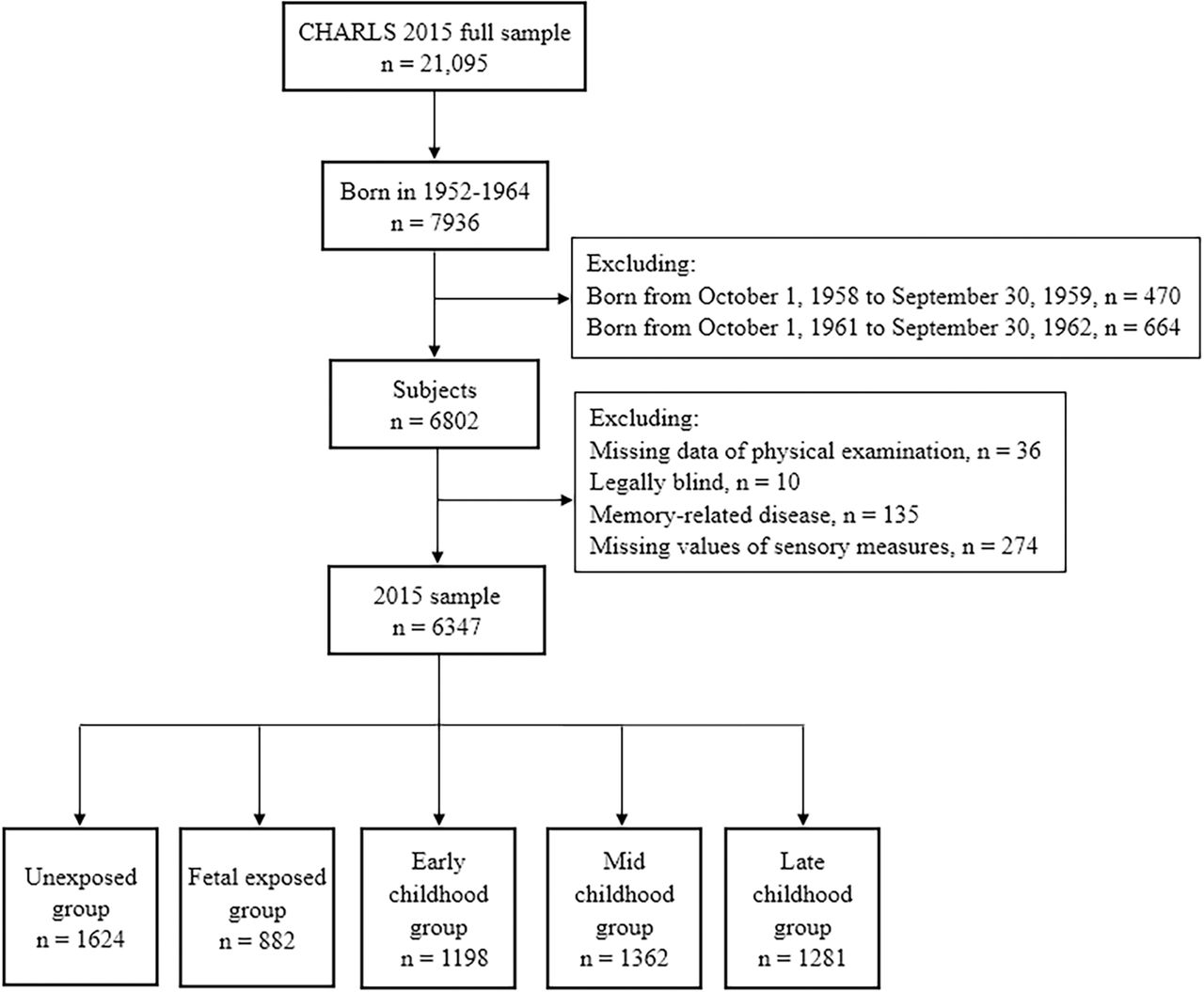
{kind=link}
Flow chart of sample selection from 2015 China Health and Retirement Longitudinal Study (CHARLS) survey.
Due to undefinable starting and ending dates of the Chinese famine, respondents born between 1 October 1958 and 30 September 1959, and between 1 October 1961 and 30 September 1962 were excluded to minimise misclassification. Following the method used in the previous Chinese famine study,11 excess death rate (EDR) of each province was used as a proxy for famine severity. Taking 100% EDR as the threshold, severity of famine-affected areas was determined at the provincial level, so as to distinguish the respondents in each of the five exposure cohorts into severely or less- to severely famine-affected populations.
Assessment of sensory functions
Similar to the Survey of Health in the USA, the presence of sensory impairments in CHARLS was measured using self-reported assessment of visual and hearing functions. Visual function was assessed using two questions: ‘How good is your eyesight for seeing things at a distance, like recognising a friend from across the street (with glasses or corrective lenses if you wear them)? Would you say your eyesight for seeing things at a distance is excellent (1), very good (2), good (3), fair (4) or poor (5)?’ and ‘How good is your eyesight for seeing things up close, like reading ordinary newspaper print (with glasses or corrective lenses if you wear them)? Would you say your eyesight for seeing things up close is excellent (1), very good (2), good (3), fair (4) or poor (5)?’. Hearing function was evaluated using the question: ‘Is your hearing very good, good, fair, poor or very poor (with a hearing aid if you normally use it and without if you normally don’t)? Would you say your hearing is excellent (1), very good (2), good (3), fair (4) or poor (5)?’. Based on the answers to the three questions, we categorised respondents as having visual or hearing impairment if they reported having fair or poor vision (for either distance or near vision) or hearing function.12 In line with the Health and Retirement Study Cohort study,13 we defined four states of sensory impairments as follows: no impairment, visual impairment but no hearing impairment, hearing impairment but no visual impairment and dual sensory impairments.
Assessment of covariates
Respondents’ sociodemographic characteristics, health behaviours and health conditions were measured in CHARLS face-to-face interviews by trained interviewers. The covariates included age, gender, education level, smoking status, alcohol consumption status, marital status (married and cohabitation, or otherwise), Hukou status (urban or rural), self-reported general health status, depressive symptoms and chronic disease conditions. Education level was categorised as ‘illiterate’, ‘primary or middle school’ and ‘high school and above’. Regarding self-reported health status, including both current conditions and status in childhood, ‘excellent’, ‘very good’ and ‘good’ were defined as ‘good’, whereas ‘fair’ and ‘poor’ were defined as ‘poor’. Depressive symptoms were estimated by Center for Epidemiologic Studies Depression Scale-10 score, which indicates clinically significant depressive symptoms.14 Chronic disease conditions were detected using the presence of chronic diseases based on self-reported doctor-diagnosed diseases, including hypertension, diabetes, dyslipidemia, stroke, kidney disease, asthma, chronic lung diseases, liver disease, stomach diseases and heart problems.
Statistical analysis
In the present study, continuous variables with non-normal distribution were reported as medians (IQRs), and discrete variables were presented as percentages (%). We performed Kruskal-Wallis test to compare the difference in skewed parameters and 𝜒2 test or Fisher’s exact test to compare the frequencies of categorical variables. The Dunnett corrections were adopted to perform post hoc comparisons with the unexposed group.
The generalised linear model (GLM) was used to estimate the association between fetal period and multi-stage childhood famine exposure and the risk of visual, hearing and dual sensory impairments in adulthood. The unexposed group was considered as the reference. Age, gender, education, famine severity, smoking, drinking, depressive symptoms, self-reported current health conditions, health status in childhood, hypertension, diabetes, chronic lung disease and heart diseases were included as control variables in the analyses. In view of the spouse data collected in CHARLS, we corrected the family cluster by adding a cluster (household) in the GLM. In addition, we conducted stratified analyses according to famine severity to distinguish severely and less severely famine-affected areas more appropriately. The interaction between famine-affected areas and different life stages of famine exposure was tested using a multiplicative factor in the logistic regression model. GLM results were reported as ORs with 95% CIs. All statistical analyses were conducted using STATA, version 13.0 (StataCorp., College Station, TX, USA).
RESULTS
Table 1 shows the demographic and clinical characteristics of participants in this study. In total, 3268 females and 3079 males were included. Of the total study sample (n=6347), 882 (13.9%) participants were exposed to the famine during the fetal period, and 3841 (60.5%) were exposed during childhood. Compared with unexposed individuals, participants in early life-exposed groups had lower education levels, and those in childhood-exposed groups had higher prevalence of hypertension, diabetes and heart diseases. Moreover, late childhood-exposed individuals were less likely to drink, and more likely to report poor health status, have chronic lung diseases and have depressive symptoms. Meanwhile, the prevalence rate of diabetes in the fetal-exposed group was higher than that in the unexposed group after Dunnett corrections.
General characteristics of study population by Chinese famine exposure
Table 2 provides the results of sensory function measures in five famine-exposed groups. After Dunnett corrections, participants in mid and late childhood-exposed groups had higher prevalence of self-reported hearing impairment and dual sensory impairments than those in the unexposed group. Compared with the unexposed group, while the prevalence of self-reported visual impairment was higher in fetal- and childhood-exposed groups, significance was not shown after Dunnett corrections.
Performance of sensory function measures by Chinese famine exposure
Table 3 indicates the relationship between famine exposure and subsequent self-reported visual and/or hearing impairment in multiple GLM. Compared with the unexposed group, the participants of late childhood-exposed group had higher risk of visual impairment, hearing impairment and dual sensory impairments, after adjusting for age and gender. Meanwhile, the mid childhood-exposed group had a risk of hearing impairment. Further adjusted for other control variables, the famine–sensory function association disappeared between both late childhood exposure and dual sensory impairments, and mid childhood exposure and hearing impairment. Interestingly, participants exposed to the famine during the fetal period had a significantly higher risk of hearing impairment (OR 1.54, 95% CI 1.06 to 2.24) and dual sensory impairments (OR 1.45, 95% CI 1.00 to 2.11) than the unexposed group. The risk of hearing and dual sensory impairments for late childhood-exposed participants was 1.75 (95% CI 1.23 to 2.50) and 1.59 (95% CI 1.09 to 2.21), respectively. However, the association between self-reported visual impairment and famine exposure was not observed in the fully adjusted model.
Multiple GLM estimates of the association between famine exposure and sensory impairments in 2015
In order to control the potential effect of age on the association between famine exposure and sensory impairment risk, we further conducted stratified analyses by famine severity (table 4). In severely famine-affected areas, the early, mid and late childhood-exposed groups had higher risk of hearing and dual sensory impairments. No significant association was observed between hearing or dual sensory impairments and famine exposure in less severely famine-affected areas, and visual impairment was not found to be related with famine exposure in both severely and less severely famine-affected areas. In addition, no significant interactions were found between famine severity and different life stages of famine exposure on prevalence risk of visual, hearing and dual sensory impairments.
Association between famine exposure and sensory impairments stratified by famine severity
DISCUSSION
Using a nationally representative sample of 6347 community-dwelling Chinese adults, our study underlined that famine exposure during the fetal period, and childhood was associated with hearing and dual sensory impairments in adulthood.
This study provides new evidence to the ‘developmental origins of health and disease’ (DOHaD) theory that early life stages may be crucial time windows for adult diseases.15 Recent famine studies suggested that undernutrition during gestation could accelerate later-life cognitive decline and ageing,16 17 and the reason may lie in affected brain size, brain perfusion parameters and premature brain ageing.18 Our previous study also suggested that early-life famine exposure might be associated with general cognition and visuospatial episodic memory in midlife.19 It was reported that hearing, visual and olfactory impairments are individually associated with cognition, and sensory impairment in midlife may be a marker of cognitive decline.20 However, there was limited evidence on the association between early-life malnutrition and adult sensorineural health. The United Kingdom Biobank study was the first to investigate the link between birth weight and late-life sensory problems, and suggested that abnormally large or small birth weight was significantly associated with poorer performance of cognitive and sensory function test.4 However, self-reported birth weight adopted in this study could potentially underestimate the association due to recall bias. Meanwhile, the everlasting adverse effects of prenatal malnutrition on late life were mainly due to underdeveloped organs and systems in early critical periods, instead of the altered body size at birth.21 22 In this study, we improved the generalisability of our findings by setting fetal and multi-stage childhood famine-exposed cohorts.
Our findings revealed that exposure to Chinese famine during the prenatal period and late childhood increased the risk of hearing and dual sensory impairments in late life. Together with our previous findings,19 23 it was indicated that the starting point of hearing, vision and cognition impairments in midlife could date back to younger age. Our results showed that the prevalence of hearing and dual sensory impairments in the fetal-exposed group was higher than that in the unexposed group (although the difference was not statistically significant in table 2). We still found the associations between fetal famine exposure and hearing or dual sensory impairments after adjusting for control variables (table 3). Studies on the 1944–1945 Dutch famine have demonstrated that nutritional deprivation during prenatal period might increase nervous system anomalies at birth and thus cause irreversible brain damage.24 Malnutrition at that time might be associated with impaired brain functioning and neurotransmitter release.25 Although the interactions between famine severity and early-life famine exposure on the risk of visual, hearing and dual sensory impairments were not significant in the current study, the associations between early, mid and late childhood famine exposure and late-life hearing and dual sensory impairments were stronger among those exposed to severer famine. The results strongly support the ‘first 1000 days’ theory25 and indicated that fetus stage and childhood (age of 0–9 years) are particularly vulnerable time periods of malnutrition reprogramming.
What attributes to this association between famine exposure and late-life sensory function decline? The Minnesota Starvation Experiment and 1944–1945 Dutch famine studies have shown that famine exposure may increase the susceptibility to chronic non-communicable diseases, such as diabetes, dyslipidaemia and anaemia.26 27 These chronic non-communicable diseases are recognised as dominant factors of cognitive and sensory function decline in midlife, with potential mechanism involving DNA methylation and cholesterol metabolism.28 The Genomic Research of the Chinese Famine study in China demonstrated that early-life exposure to severe famine could increase methylation in the insulin-like growth factor 2 gene, which would consequently increase cholesterol amount in midlife.29 Animal evidence proved that food restriction from weanling to 42 days of life among male Wistar rats could decrease glutamate release in the cortex, hippocampus, midbrain and brainstem at 370 days of life.30 It was indicated that malnutrition during critical periods of brain development caused an irreversible adverse effect on the auditory primary sensory pathway.30
The present study suggested that famine exposure in the fetal period and late childhood was positively associated with hearing and dual sensory impairments rather than visual impairment. Interestingly, although famine exposure was also reported to worsen visual-motor performance in late life,31 the association between famine exposure and risk of visual impairment did not reach statistical significance in the current study (though negative). This inconsistency may originate from different visual function assessment measures and different postnatal stages of famine exposure, and more detailed investigations can be conducted in the future. Meanwhile, it has been proven that the main causes of hearing impairment among Chinese elderly people are chronic diseases, presbycusis, long-term exposure to noise, otitis and media,32 and the occurrence of dual sensory impairments is positively associated with chronic diseases, depression, anxiety and cognitive impairment, especially for the elderly.12 33 The above-mentioned reason could partly explain the phenomenon that famine–sensory function association was insignificant in terms of visual impairment but significant in terms of dual sensory impairments. However, we should be cautious about the generalisability of the main findings.
In the analysis of famine–sensory function associations, there exists potential bias caused by the use of hearing and vision measures, which allows for spectacles or hearing aids. The adoption of medical devices such as spectacles or hearing aids may make contributions to sensory rehabilitation,34 but in current times in China, only a small portion of adults with visual and/or hearing impairment use them to improve their sensory functions. The CHARLS 2013 data set suggested that for Chinese residents aged 60 years and above, only 10% visually impaired participants and 0.8% hearing impaired participants wore medical aids regularly.35 The use rate of aids was much lower than expected in China, suggesting that we could minimise the effects of aid use bias in the current study.36 Possible reasons for the low uptake of aids include financial constraints, misinformation and mistaken views (eg, spectacles may worsen vision loss, or hearing impairment is normal in the ageing process).37
Our study had several limitations. First, the use of self-reported measures to estimate sensory functions could potentially underestimate the association between famine exposure and sensory impairments, though this method has been widely adopted in epidemiological studies to assess visual and hearing functions.12 13 Second, using date of birth to define famine exposure might result in misclassification of exposed groups, but identifying an unexposed group not affected by famine was not feasible because the Chinese famine affected nearly the whole China. Finally, we used provincial EDR estimated from government reports as the proxy for famine severity, which may be subject to falsification, but EDR is still one of the most commonly used famine severity measures in China.
CONCLUSIONS
In conclusion, this national cohort study is among the first to estimate the long-term sensory function consequences of early-life famine exposure in a non-European population, suggesting that exposure to famine during the gestation period and late childhood has everlasting adverse effects on hearing impairment and dual sensory impairments in adulthood. The study highlights the importance of providing sufficient nutrition during the critical earliest stages of development.
What is already known on this subject
Existing research suggests that early-life malnutrition pregnancy and infancy malnutrition played an important role in susceptibility to later non-communicable diseases .
However, little is known about the association between severe nutritional deficiency during early-life and midlife sensory functions.
What this study adds
Severe nutritional deprivation during prenatal and postnatal periods has everlasting adverse effects on hearing and dual sensory impairments in Chinese adults in their early 50s.
This national cohort study highlights the importance of providing sufficient nutrition during the critical earliest stages of development to promote healthy ageing.
Acknowledgments
The authors are grateful to the China Health and Retirement Longitudinal Study (CHARLS) team for providing data and simple training in using the database.
REFERENCES
Footnotes
Contributors HF designed the study. HR and HF carried out the data analyses. All authors discussed the analysis results, wrote the manuscript, and read and approved the final version of the manuscript.
Funding This work was supported by the National Natural Science Foundation of China (grant number 71774006)—awarded to HF and China Postdoctoral Science Foundation (grant number 2019M650392)—awarded to HR.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open-access repository.