Article Text

Abstract
Background Little is known about the impact of socioeconomic status (SES) on incidence of stroke in China. This study aimed to examine the association of SES, which was measured by different indicators, with incidence of stroke and gender differences in the association.
Methods and results Two prospective cohort studies were conducted including 2852 participants aged ≥60 years in Anhui province and 3016 participants in four other provinces in China. During a median follow-up of 7.1 years, 211 incident stroke cases occurred in the Anhui cohort. The risk of stroke increased with living in rural areas (adjusted HR 2.49, 95% CI 1.19 to 5.22; women 3.64, 95% CI 1.17 to 11.32, men 2.23, 95% CI 0.81 to 6.19), but not significantly with educational level, occupational class, satisfactory income and financial problems (except for women with low education). The four-province cohort had 113 incident stroke cases over the 3.1 years’ follow-up. The five SES indicators were not significantly associated with incident stroke (except for increased risk in men with high occupation), but additional measurement for actual income showed that incident stroke increased in women with low personal income and in men with high family income. Pooled data from the two cohorts demonstrated the impacts of rural living (1.66, 95% CI 1.08 to 2.57) and having high occupational class (1.56, 95% CI 1.01 to 2.38), and gender differences for women with low education (2.26, 95% CI 1.19 to 4.27).
Conclusions Rural living and being female with low SES are associated with increased stroke risk in China. Strategies to improve public health in the rural communities and gender-specific targets for health inequality should be an integral component of stroke interventions.
- socio-economic
- inequalities
- stroke
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The burden of stroke has increased across the world, with the disability-adjusted life-years ranked at third up from fifth over the past 30 years.1 Previous studies2–4 showed that low socioeconomic status (SES) was associated with increased incidence of stroke in the general population. The global burden of disease study5 demonstrated that people in low and middle-income countries (LMIC) have a higher risk of stroke than in high-income countries (HIC). Current knowledge of the impact of SES on incident stroke has been predominantly derived from HICs, which may not be applicable to those in LMICs. There are fewer studies undertaken in LMICs to assess the association of SES with incident stroke.
China is the largest LMIC and has the highest estimated lifetime risk of stroke worldwide.6 There are around 5.5 million new stroke cases occurring in China each year.5 Over the past decades, China has experienced rapid economic growth, along with an increasing gap in income between rich and poor.7 However, it is not known whether socioeconomic inequalities, including urban-rural differences,7 are associated with increased risk of stroke.
Previous studies in HICs showed some inconsistent findings of the association between SES and incident stroke.3 8 No study has assessed the impacts of different SES indicators on incidence of stroke simultaneously. Most of the studies did not adjust for other SES variables when examining incidence of stroke in relation to one measurement of SES.3 4 9 Few studies have investigated gender differences in the association of SES with incident stroke. In this paper we examine data from two community-based cohort studies in China to assess the impacts of multiple measurements of SES on the incidence of stroke and their gender differences.
Methods
Studied populations were derived from the Anhui cohort study and the four-province cohort study in China.
Anhui cohort study
The methods of the baseline investigation and the follow-up in the Anhui cohort study have been fully described previously.10 Briefly, we randomly selected 1810 people aged ≥65 years who had lived for at least 5 years in Yiming subdistrict of Hefei city in 2001 and 1709 aged ≥60 years from all 16 villages in Tangdian district of Yingshang county in 2003. A total of 3336 older people participated in the study (urban n=1736), with a response rate of 94.8%. Informed consent was obtained from each participant. In the case of those who were unable to provide informed consent such as due to disability or limited education level, their next of kin or caregivers were invited to provide assent for participation.11 The participants were interviewed at home by a trained survey team from the Anhui Medical University.
The main interview materials were a general health and risk factors questionnaire, and the Geriatric Mental Status (GMS)—a comprehensive semistructured mental state interview.12 In the general health and risk factors record, we collected data relating to sociodemography, social networks and support, psychosocial aspects, cardiovascular disease (CVD) and other disease risk factors.10 12 We documented stroke from participants’ self-report of having being diagnosed by a doctor.13 In older people self-reported doctor’s diagnosis of stroke has been validated14 and our previous study showed that these older people with stroke had an HR of 1.91 (95% CI 1.45 to 2.52) for 5-year mortality compared with their non-stroke counterparts.13 Using the GMS interview data and the Automated Geriatric Examination for Computer Assisted Taxonomy12 we diagnosed depression and dementia for each participant. According to standard procedures10 we measured systolic and diastolic blood pressure, weight and height, and waist circumferences for all participants at baseline interview (wave 1).
Baseline SES measurements
We measured SES from long-term residential location in urban and rural areas and from individual records of educational attainment level, occupational class, satisfactory income and a serious financial problem in the past 2 years.13 In the interview we asked each participant whether he or she attended any school or not. If answered with ‘yes’, they would be asked to specify either (1) primary school, (2) secondary school, (3) high secondary school/professional school or (4) university/college. Those without any formal school attainment were defined as illiterate. All participants gave their occupational class according to their current or last main job titles as a peasant, manual worker, officer/teacher, businessman, housewife or other. We asked each participant the questions ‘Are you satisfied with your income?’ (with answers either at ‘very satisfied’, ‘satisfied’, ‘average’ or ‘poor’) and ‘Have you had any financial problems in the past two years’ (with answers ‘yes’ or ‘no’).
Follow-up of cohort
One year after the baseline survey we reinterviewed 2608 participants (wave 2) using the same protocol as at baseline. From 2007 to 2009 we successfully re-examined 1757 cohort members (wave 3), and in 2010–2011 we carried out a wave 4 survey on surviving cohort members and reinterviewed 944 participants.10 In waves 3 and 4, we added in the 10/66 dementia algorithm research package and more risk factors including dietary intakes, passive smoking and personal and family incomes.11 At each wave interview of the follow-up we documented incident stroke based on self-reported doctor diagnosis of stroke.
The vital status of the cohort members was monitored until December 2011. At each survey wave we conducted home visits to obtain information about participants’ survival status through multiple sources including resident committees, family members, neighbours and friends. In total we identified 671 deaths during the follow-up of the cohort. Using a standard verbal autopsy questionnaire we interviewed the next of kin responsible for the deceased or reviewed the death certificate to ascertain causes of death,12 including stroke diagnosis.10 13
Four-province study
Using the same protocol as that in the Anhui study wave 3, we carried out a large-scale community-based household survey in four provinces of China (Guangdong, Heilongjiang, Shanghai and Shanxi) in 2008. Their methods of the baseline investigation have been fully described previously.11 In brief, we randomly recruited no fewer than 500 residents aged ≥60 years from the urban and rural communities separately from each province. In total, 4314 participants completed the interview in 2008–2009, with an overall response rate of 93.8%. We documented cardiovascular diseases and risk factors (CVDRF) and SES variables for each participant.11
In 2010–2012 we followed up the cohort, having identified 259 deaths and reinterviewed 2892 survivals using the same questionnaire as that at baseline.
Statistical analysis
In the Anhui cohort study, we analysed the data from 2852 cohort members, after excluding 141 participants with stroke at baseline and 343 who were lost to follow-up. In the four-province cohort study, the data from 3016 cohort members were analysed, after excluding 166 participants who had stroke at baseline, 1102 who were lost to follow-up and 30 who had no SES indicator measured. We computed person-years at risk for cohort members to the end of follow-up, date of incident stroke, death or loss at follow-up. Annual incidence rate was expressed as cases per 1000 person-years. We described baseline characteristics and CVDRFs of participants using mean (SD) and percentage (%) and examined differences in their distributions between women and men at baseline using a one-way analysis of variance for continuous variables and a χ2 test for categorical variables. We grouped individual SES variables into (1) low, (2) middle, and (3) high levels; in Education: (1) illiterate, (2) primary school, and (3) secondary school or higher; in Occupational class: (1) peasant, (2) manual labourer or housewife, and (3) official/teacher or business/other; in Satisfactory income: (1) poor or average, (2) satisfactory, and (3) very satisfactory. The financial problem in the past 2 years was recorded as ‘yes’ or ‘no’. In the four-province study, we divided baseline annual personal income and family income into three groups according to their respective tertile cut-off points.
We employed multivariate adjusted Cox regression models to examine the risk of incident stroke in relation to each of SES indicators in the two cohorts, respectively. We calculated the HR and its 95% CIs for incidence of stroke. In the models we adjusted for age, sex, body mass index, smoking, alcohol consumption, marital status, frequency of visiting children/other relatives, hypertension, heart disease, diabetes, activity of daily living (ADL), and depression and dementia. When the covariables had missing data, we took them as a separate group for analysis. Apart from examining the independent effect of one SES indicator from other SES we included all other SES indicators in the models for full adjustment. In the full model data analysis, we investigated the impacts in women and men separately, and tested their gender differences using a ratio of 2 HRs as we did before.12
We pooled the two-cohort findings where possible using a meta-analysis method as we did before13 to assess the impacts of different SES measurements on incidence of stroke, so as to increase statistical power. All analyses were performed using SPSS V.24.0 (SPSS) and Stata V.14.0 (StataCorp, College Station, Texas, USA).
Results
Anhui cohort study
Of 2852 participants, the average age was 71.7 years (SD 6.9), 51.8% were women and 48.2% lived in rural areas. The distribution of baseline characteristics of participants is shown in online supplementary table 1. Compared with men, women were more likely to have low levels of education, occupation and satisfactory income, be obese, be widowed and have high levels of depression and dementia, but were more likely to have never smoked, not drink, live with children and/or grandchildren and be visited daily by children or other relatives. There were no significant gender differences in age, urban rurality, financial problem, ADL and cardiovascular comorbidities.
Supplemental material
Over the 10 years’ follow-up, 211 cases of stroke were identified. Table 1 shows the numbers, incidence and adjusted HRs of stroke in participants living in urban and rural areas. The HR for stroke in participants living in rural areas was significantly increased with adjustment for different sets of confounders, including other SES indicators. Separate data analysis for women showed a fully adjusted HR of 3.64 (95% CI 1.17 to 11.32) and for men 2.23 (95% CI 0.81 to 6.19) (table 2).
Number, rate and HR of incident stroke in older people from urban and rural areas in China: the Anhui cohort study
HRs of incident stroke by socioeconomic status in women and men: the Anhui cohort study
There were no significant associations of education, occupation, satisfactory income and financial problem with incident stroke, although increased HRs in participants with low levels of education and occupation and a financial problem were significant before adjustment for other SES (online supplementary table 2). However, separate data analysis by gender showed that there were significantly increased risks of stroke in women with low education (table 2).
Four-province cohort study
Of 3016 participants, 113 cases of incident stroke occurred over the 3 years’ follow-up. Compared with those living in urban areas, participants in rural areas had a fully adjusted HR of 1.34 (95% CI 0.78 to 2.30) of incident stroke (online supplementary table 3). There were no significant associations of education, satisfactory income and financial problem with incident stroke, except for high occupational class appearing associated with increased stroke (online supplementary table 3). Separate data analysis for women and men showed findings similar to those for the combined sample and there were no gender differences in these associations (data not shown), except for men with high occupation having increased the risk of stroke (2.17, 95% CI 1.08 to 4.35) (table 3).
HRs of incident stroke by occupational class in women and men: the four-province cohort study
Table 4 shows the numbers, incidence and adjusted HRs of stroke in participants with different levels of annual personal and family incomes. Significantly increased risk of incident stroke was seen in women with low annual personal income (3.05, 95% CI 1.17 to 8.00) and in men with high family income (2.38, 95% CI 1.14 to 4.76 vs middle income; p=0.037 in three group differences).
Number, rate and HR of incident stroke in older people with actual income in China: the four-province cohort study
Pooled data from the Anhui cohort and the four-province cohort
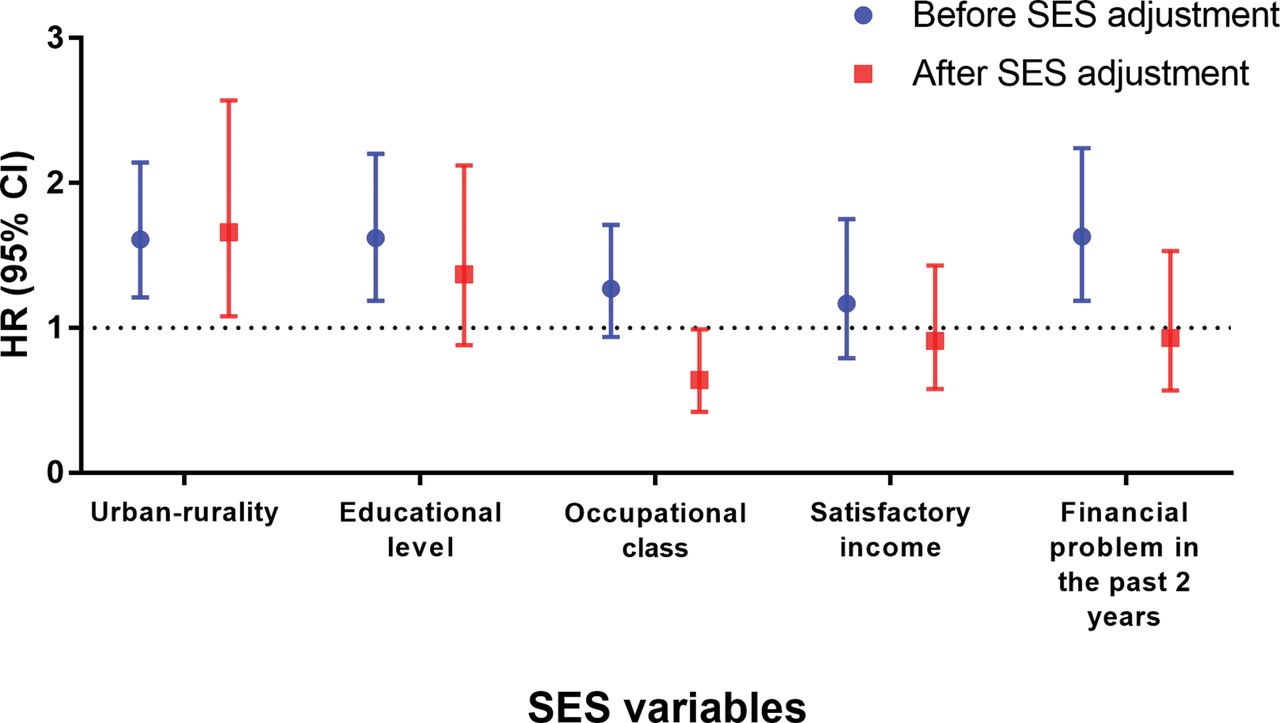
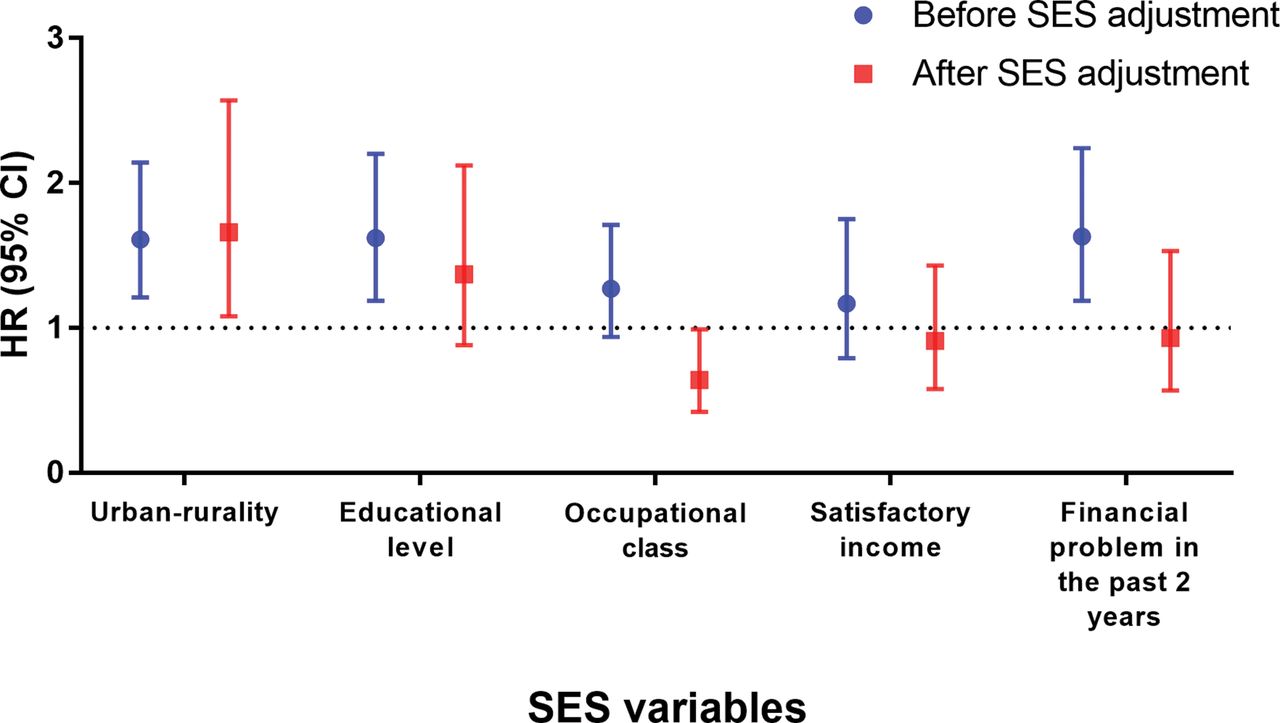
Figure 1 shows pooled data of HRs of incident stroke in people with low SES from the two cohorts. There was a significantly increased risk of stroke in participants living in rural areas, before and after adjustment for other SES variables. The associations of low education and financial problems with incident stroke were significant in the analysis before adjustment for other SES variables. High occupational class was associated with increased risk of stroke after adjustment for other SES variables. Other HRs in figure 1 were not statistically significant.
{kind=link}
Pooled HRs for the risk of incident stroke in low socioeconomic status (SES) before and after adjustment for SES from the Anhui cohort and the four-province cohort studies.
Pooled data for women and men separately showed that women with rural living or low education had significantly increased risk of stroke, and other HRs were not statistically significant (table 5). There were no gender differences in the associations of rural living, education, occupation, satisfactory income and financial problems with incident stroke (table 5).
Pooled HR of incident stroke in different SES indicators among participants from the Anhui cohort and the four-province cohort studies
Discussion
Our community-based cohort study examined the impact of different measurements of SES on incidence of stroke in China. It demonstrated that inequality in the risk of stroke was largely for people who lived in rural areas. Women who had low education or low personal income also had increased risk of stroke, as did men with high occupational class or family income.
The association of low education with increased risk of stroke has been observed in the HICs.15 In Australia women with least education versus highest education had increased risk of stroke.16 Our study also found that women with illiteracy had significantly increased risk of stroke compared with their counterparts who attained at least primary school. However, our data from the male population did not show a significant association of low educational level with increased risk of stroke. It may be because other factors, for example, smoking and alcohol drinking in Chinese men, play a more important role in the aetiology of stroke, covering the impact of low education on risk of stroke.
Our study showed that high level of occupational class was associated with increased incidence of stroke, mainly in men. This is different from those in previous studies undertaken in HICs.4 One of the reasons for it could be attributed to epidemiological transition in the early stages that those with high occupational class are more likely to have adverse lifestyles including smoking17 and drinking,18 sedentary behaviour19 and psychological stress,20 especially men. These lifestyles are associated with increased risk of stroke.
Our data of the four-province study showed that men with high family income had an increased risk of stroke in comparison to their counterparts with low and middle family income. This could be explained by lifestyle changes among them; the Chinese men with high income experienced and adopted unhealthy lifestyles, such as smoking and drinking alcohol.21 The pattern of high income associated with high risk of stroke was also observed in HICs. In USA, the incidence of stroke in people aged above 75 was increased with higher income (HR 2.33, 95% CI 1.16 to 4.55).3 In France, the Three-City Study demonstrated that in those aged over 65 years there was an 80% increased risk of ischaemic stroke in those with higher income compared with lower income (HR 1.77, 95% CI 1.20 to 2.61).9 In our study, high income is partly in line with high occupational class, and to a large extent a man’s earnings and occupation would determine his family’s SES. Therefore, the explanations relating to some risk factors for incident stroke in high occupational class also could be applied to men with high family income.
The current study did not find a significant association of satisfactory income or financial problem with incidence of stroke. Satisfactory level of income involved people’s feeling about income, while the financial problem in the past 2 years reflected ‘the financial crisis’. These proxies could be good for examining the risk of mental disorders and other chronic diseases.22 23 In this study, we analysed the data of the actual income from the four-province study and found that older women with low personal income had increased risk of stroke. The finding is consistent with other studies.24
Compared with other indicators of SES above, the impact of the rural-urban disparity on incident stroke has rarely been studied. Based on existing literature, we have found few published studies of examining differences in incidence rate of stroke between rural and urban areas. In a large-scale population-based cohort study in Portugal, Correia et al examined the data from an older population aged 65+ years and found that the annual incidence of stroke per 1000 population was higher in rural (from 9.5 to 20.2) than in urban areas (from 6.8 to 10.9).25 Data from young and middle-aged populations in a study in China also showed that incidence of stroke in rural areas was significantly greater than that of their urban counterparts.26 However in sub-Saharan Africa, a community-based study of the Tanzania Stroke Incidence Project found that there was higher incidence of stroke in older people living in urban versus rural areas, which could be due to high prevalence of stroke risk factors at a community level in the urban region.27 In spite of these differences between rural and urban in the incidence of stroke, all three studies did not adjust for confounders to assess the rural-urban disparities in the risk of stroke, and the residual effects could therefore not be removed. Our study, with adjustment for many important confounders, showed that older people living in the rural areas in China had significantly increased risk of stroke.
There was a wide inequality between rural and urban in China due to disparities in education, employment opportunities, income, political rights, social welfare and healthcare services.7 In rural areas some risk factors for stroke were common and uncontrolled.26 A health survey in China showed that people living in rural areas had higher prevalence of hypertension and that they were particularly unaware, leaving high levels of untreated and uncontrolled hypertension.28 Primary care and preventive care access remain poor in rural areas,29 including lack of facilities such as CT or MRI scan for the diagnosis of stroke.30 People who live in rural areas might not receive adequate preventive interventions for high-risk factors and thus would have increased risk of stroke.31 These could be some possible explanations for an association of living in rural areas with increased incidence of stroke.
In China, apart from the rural-urban inequality, low income has been associated with reduced healthcare use. Luo et al found that compared with those from lower income families, people from higher income families were more likely to use outpatient services (OR 1.55, 95% CI 1.05 to 2.29) and inpatient services (1.40, 95% CI 1.00 to 1.98).32 Previous studies showed that there were no gender differences in outpatient visits, but among those with low income women used outpatient services more frequently than men.32 These could partially explain the findings of the current study.
Our study has identified that women were more evident in the disparities of incident stroke in terms of levels of education and income, apart from rurality. The women in our study were born in a turbulent age when most of them had no opportunities to attain schooling and work outside due to many factors, for example, poverty, Chinese tradition. Also, female education was rarely given priority due to poverty and patriarchal attitudes,33 thus causing a high illiterate rate in older women.34 Older women in China are still among the most economically disadvantaged population groups. Consequently, once they experienced some economic problems, they would have increased risk of incidence of stroke.
Strengths and weaknesses of the study
The main contribution of this study, beyond the intrinsic importance of studying inequality in stroke risk in the largest and most populous LMIC, lies in what it tells us about the simultaneous impacts of multiple measurements of SES on incidence of stroke and their gender differences. As far as we know, our study is the first to report gender differences in the association of SES with incident stroke, addressing that women had higher inequality in incidence of stroke in relation to low SES. Our study included important covariables for adjustment such as ADL and depression and thus the confounding effect would be minimised. Particularly, we adjusted for each of these SES indicators (rurality, education, occupation and income), and thus their residual effects from other SES indicators were removed. Our study has limitations. First, although each of the two cohorts has enough participants to examine incidence of stroke in relation to SES, multiple adjustment analysis gave HR estimates a wide 95% CI, reducing the statistical significance. However, our pooled data could increase the study power. Second, we do not have data of stroke subtypes in the cohort for analysis, and it is unclear whether or not there were significant differences in the impacts of SES on ischaemic and haemorrhagic strokes. However, studies in other countries showed similar effects of SES on incidence of ischaemic and haemorrhagic strokes.35 36 In China the prevalence of hypertension and the proportion of intracerebral haemorrhage (ICH)26 are higher than those in Western countries,37 and previous studies suggested that hypertension has more effects on increased risk of ICH than on acute ischaemic stroke.38 It is unclear what the effects are of both prevalent hypertension and ICH on the association between SES and incident stroke in this study. However, we adjusted for multiple CVD risk factors, including hypertension in the data analysis, and thus the confounding effect of hypertension on the association has been minimised. Nevertheless, we need further studies focused on this issue in China, including detailed data collection using brain scan for stroke subtypes to clarify the effects of these SES indicators on the incident risk of each stroke subtype. Third, in the two cohorts we analysed self-reported satisfactory income associated with incident stroke. The satisfactory income is the person’s perception of her/his own income and not the actual income. Although there is significant correlation between this measurement and actual salary income (online supplementary table 4), we did not find its association with risk of stroke. However, in the four-province cohort we used actual income from personal and family and found their associations with incident stroke in women and men. Fourth, the four-province cohort study had a 27% loss to follow-up rate. This was because during that period China had many residential area houses reformed and rearranged due to rapid development, and some participants moved home and we could not trace their new house address. In the Anhui cohort, we also had a number of cohort members lost to follow-up, for example, at wave 3 only 1757 were reinterviewed (excluding 565 deaths), which gave a 30% loss to follow-up rate, although the overall loss to follow-up rate across the Anhui cohort wave 2–4 interviews and identified mortality was lower (10.7%).12 We do not know whether those lost to follow-up had higher or lower level of incident stroke than other cohort members. The bias, if any, could be in any direction for the association of SES with incident stroke. However, the loss to follow-up rate in our study is similar to those in some studies undertaken in Western countries,39 and there is need of further studies with lower loss to follow-up rate to examine the association of SES with incident stroke in China. Fifth, caution should be exercised in generalising the findings to the whole population of China. The impact of SES on the risk of stroke in our cohort study consists of participants aged ≥60 years old in urban and rural communities. Those aged <60 years need to be included in further research.
Conclusion
This study demonstrates inequality in the risk of stroke in terms of SES in China. The rurality was a main resource of incident stroke inequality. There were gender differences in the impact of SES on stroke risk; in women increased risk of stroke was associated with low education and low personal income, while in men it was with high occupational class and high family income. The gender-specific strategies and preventive interventions of health promotion targeting people living in rural areas, through reducing socioeconomic deprivation, would be helpful in campaigns to reduce stroke incidence in China. Increasing public health education and improving stroke care access in rural areas, particularly in women, and constructing balanced policies for rural seniors could have large impacts in reducing the burden of stroke in China.
What is already known on this subject
Many studies in high-income countries (HIC) showed that low socioeconomic status (SES) was associated with increased incidence of stroke. There is a lack of data from low and middle-income countries and no study has been done in China where the stroke is the number one killer to examine the association of SES with incidence of stroke.
The findings of previous studies in HICs were not consistent in assessing the impact of SES on incidence of stroke. Few studies have used multiple measurements of SES to examine their associations with incident stroke simultaneously. No study has been done to investigate gender differences in the associations.
What this study adds
In China, living in rural areas was associated with increased risk of incident stroke in terms of SES.
In women, those with low levels of education and personal income had a higher risk of incident stroke than their counterparts.
In men, those with high levels of occupational class and family income had a higher risk of incident stroke than their counterparts.
Health promotion in rural areas and gender-specific targets would help reduce health inequality and incidence of stroke in China.
Acknowledgments
The authors thank the participants and all who were involved in the Anhui cohort and the four-province cohort studies. Dr Yulong Wang is the recipient of a grant from Shenzhen Health and Family Planning Commission, ShenZhen, Guangdong, China for the training of rehabilitation ability of severe stroke patients (project no. SM201623A).
References
Footnotes
Contributors RC (guarantor) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. RC obtained funding, conceptualised and designed the study, supervised the analyses and revised the manuscript. WZ had full access to all the data in the study, managed the database, performed the analyses and drafted the initial manuscript. AH, YW, XC, AC, KF and JN commented and revised the manuscript and interpreted the findings. JT, YP and DW provided statistical support and input, interpreted the data and commented on the manuscript. EB commented and supported the data analysis, interpreted the findings and provided critical revision of the manuscript. All authors approve the final version of the manuscript.
Funding The research was funded by the BUPA Foundation (grants numbers 45NOV06 and TBF-M09-05) and the Alzheimer’s Research UK (grant number ART/PPG2007B/2) for the two cohorts’ data collection.
Disclaimer The funders had no role in the study design, data analysis and interpretation, the writing of the manuscript and the decision to submit the manuscript for publication.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approvals for the Anhui cohort study and the four-province study were obtained from the Ethics Committees of University College London, and School of Health and Wellbeing at University of Wolverhampton, UK, and the Research Ethics Committee of Anhui Medical University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.