Managing chronic disease
BMJ 1999; 318 doi: https://doi.org/10.1136/bmj.318.7191.1090 (Published 24 April 1999) Cite this as: BMJ 1999;318:1090
Presents such challenges that the BMJ is devoting a special issue to it
- Ronald M Davis (rdavis1{at}hfhs.org), North American editor.,
- Edward H Wagner, Director,
- Center for Health Studies, Group Health Cooperative of Puget Sound, Seattle, Washington, USA,
- Trish Groves, Primary care editor.
Rapid improvements in health and longevity are dramatically changing the burden of illness throughout the world. In developed countries changes in lifestyle and improvements in the treatment of major causes of mortality have aged the population and increased the prevalence of chronic diseases. Poor countries that have achieved gains in life expectancy are also experiencing an increase in chronic disease as they proceed through the “epidemiological transition”—the changing pattern of health in which they inherit the problems of the rich.1
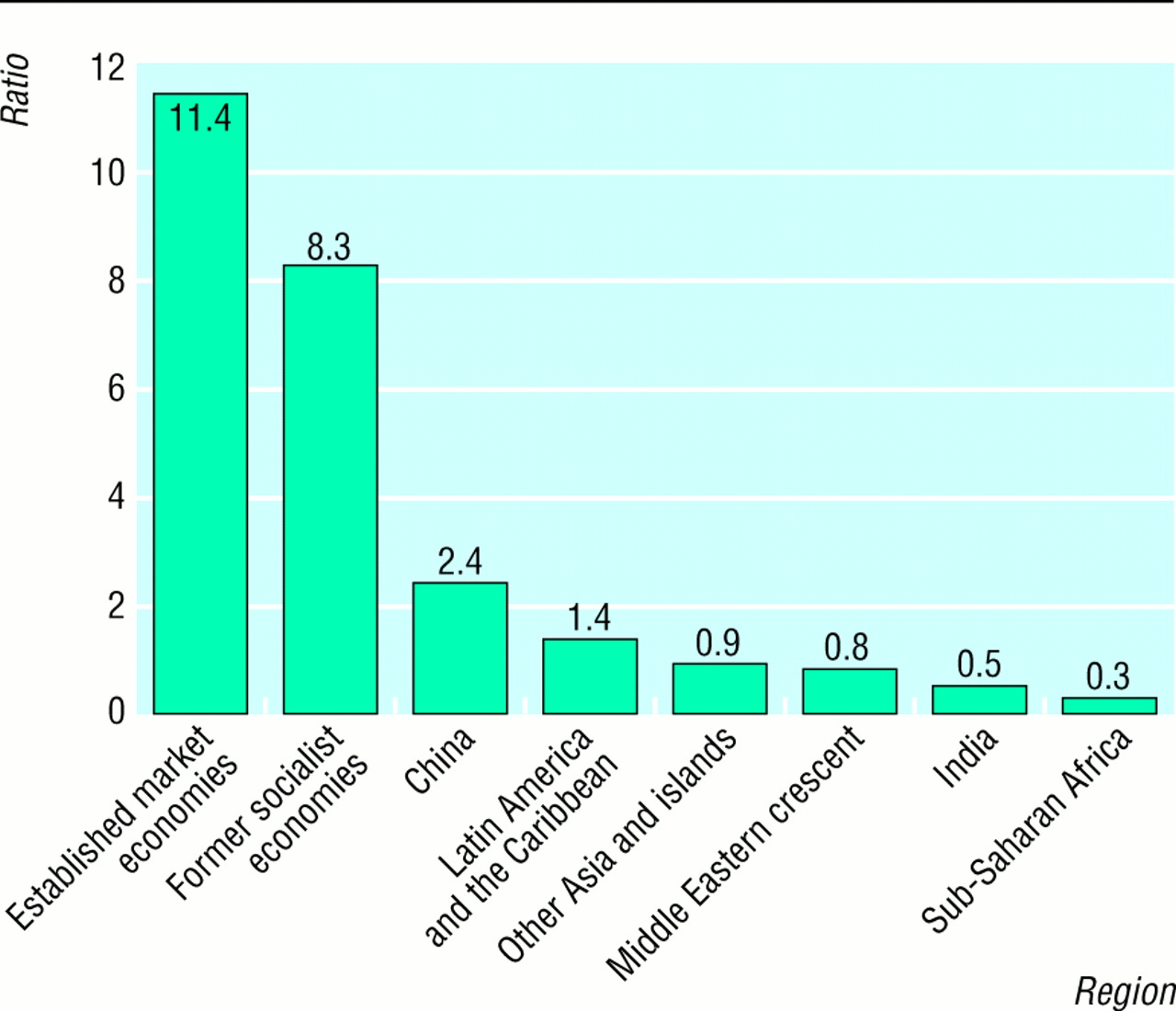
The epidemiological transition (now called the “health transition”) has progressed substantially in several developing regions. This is shown clearly in the ratio of disability adjusted life years (DALYs; the number of years lost from premature death plus the years lived with a disability) caused by non-communicable diseases to DALYs caused by communicable, maternal, perinatal, and nutritional conditions (see figure).2 The established market economies and the formerly socialist economies of Europe have essentially completed the transition. Non-communicable diseases already predominate as a cause of DALYs in China and in Latin America and the Caribbean, while “other Asia and islands” and the Middle East are close to that transition point.

Ratio of disability adjusted life years (DALYs) caused by non-communicable diseases to DALYs caused by communicable, maternal, perinatal, and nutritional conditions for different regions of the world, 19902
{kind=link}
Thus most countries are suffering from, or will soon suffer from, an enormous burden of chronic, non-communicable disease. A few statistics illuminate the burden. An estimated 691 million people worldwide have high blood pressure. The number of diabetics is projected to increase from 135 million now to 300 million by 2025. About 29 million people suffer from dementia, and 2.6 million new cases occurred in 1996. Rheumatoid arthritis affects about 165 million people.3
Obviously the prevention of chronic disease through avoiding risk factors is the prime goal, with early detection and cure (when possible) the second. But those objectives are often not met, and thus countries and their health systems need to address the challenge of managing chronic conditions. To focus attention on this topic, the BMJ will devote an entire issue to managing chronic disease in February 2000.
In North America the management of older and chronically ill patients increasingly dominates medical practice. Yet study after study, along with various performance indicators,4 show that patients often miss out on effective pharmacological and behavioural therapies and lack the information and support they need. Many subspecialists argue that generalists do not provide high quality care in chronic illness. Employers and health insurers are hiring disease management companies who “carve out” particular conditions for separate care, threatening the integrity and continuity of the doctor-patient relationship.5 The news is not all bad, however: funding agencies and researchers have turned their attention to improving the management of chronic disease. For example, the Robert Wood Johnson Foundation supports a series of programmes addressing various aspects of chronic illness management from policy development to system change to financing. Sustained improvements in managing chronic diseases require better practice systems, improvement in doctors' skills, and more effective use of non-physician providers. Practice system changes that have shown the greatest promise of success integrate self management support programmes, guideline based treatment plans, nurse case management, more intensive follow up, and registries that provide reminders and feedback.6
The same goal—high quality coordinated care that is cost effective and widely available—should in theory be more easily attained in the British NHS than in the more fragmented system in the US. And the NHS is working on it. All NHS organisations now have to practise clinical governance, a process that is meant to assure and improve quality while ensuring that professionals develop well, and are accountable for the quality of care.7 New bodies such as the National Institute for Clinical Excellence and the Commission for Health Improvement8 will help practitioners and services to deliver the evidence based care that patients need. Meanwhile new primary care structures9 and better information technology should improve the coordination of care. But all of these changes are generalised and could take years to produce gains in the population's health. Many specific interventions for patients with chronic diseases have been tested by British researchers, and not all have made much difference to patients' health.10–12 We still need much more evidence to identify the interventions and strategies that really work for patients, whether in a national health system or a more mixed health economy.
We hope the BMJ's theme issue on managing chronic disease will help disseminate research findings, encourage more research, and stimulate wider debate. In particular we invite authors to send us papers on the following topics:
clinical management of specific chronic conditions (asthma, diabetes, etc);
care of patients with multiple chronic conditions and frail elderly people;
practice based interventions that address chronic disease care—for example, informatics strategies, patient education;
system level strategies to improve the delivery of care for chronic illness;
disease prevention and risk reduction in people with chronic illness;
the integration of chronic disease management into primary care.
The Western Journal of Medicine, now co-owned by the BMJ Publishing Group, will also publish a theme issue on the topic at the same time as the BMJ's special issue. Authors should indicate whether they would like publication in the BMJ, the WJM, or both. The editors of both journals don't want to adhere to a rigid definition of “chronic” disease in considering papers for these issues. However, potential contributors may like to note the definition used by the US Centers of Disease Control and Prevention: “illnesses that are prolonged, do not resolve spontaneously, and are rarely cured completely.13
We are happy to consider reports from any part of the world and welcome original research, editorials, educational articles, debate pieces, and rigorous review articles. All manuscripts will go through the usual peer review process, and the deadline for submission is 1 August 1999.
Footnotes
-
Drs Davis and Wagner will serve as guest editors of the theme issue on chronic disease management. Drs Miriam Shuchman and Michael Wilkes, coeditors of the Western Journal of Medicine, will oversee publication of the WJM's theme issue.