Seasonal variation in coronary artery disease mortality in Hawaii: observational study
BMJ 1998; 316 doi: https://doi.org/10.1136/bmj.316.7149.1946 (Published 27 June 1998) Cite this as: BMJ 1998;316:1946
- Todd B Seto, fellow, cardiovascular diseasea (tseto{at}bidmc.harvard.edu),
- Murray A Mittleman, assistant professor of medicinea,
- Roger B Davis, associate professor of medicineb,
- Deborah A Taira, health economistc,
- Ichiro Kawachi, associate professor of health and social behaviourd
- a Cardiovascular Division, Beth Israel Deaconess Medical Center, Boston MA 02215, USA
- b Division of General Medicine and Primary Care, Beth Israel Deaconess Medical Center
- c Health Institute at New England Medical Center, Harvard Medical School, Boston, USA
- d Harvard School of Public Health, Boston, MA, USA
- Correspondence to: Dr Seto
- Accepted 22 December 1998
A seasonal variation in cardiac mortality has been noted in both the northern 1 2 and southern3 hemispheres, with higher death rates during winter than summer. Previous studies reporting seasonal variation in mortality from coronary artery disease examined data from regions with distinct seasonal changes in temperature. To determine whether seasonality in mortality exists in a tropical climate with little variation in temperature we examined the monthly mortality from coronary artery disease among residents of Hawaii.
Methods and results
Hawaii consists of six main islands, with a population of 1.1 million.4 We obtained monthly rates of deaths from coronary artery disease (ICD-9 410-414) as recorded on death certificates during 1984-93 from the state of Hawaii. All non-residents of Hawaii were excluded. Because the likelihood of a diagnosis of a respiratory infection might vary by season, we used mortality from respiratory infection (ICD-9 480-487) as a proxy for incidence of respiratory infection. We used the average 24 hour temperature and hours of sunlight in Honolulu for each year as an estimate for the entire state.
We used the Cochrane-Orcutt regression analysis to test for annual periodicity. Results were fitted to the equation: y=b0+b1 x cos(2π x month/12)+b2 x sin (2π x month/12). Goodness of fit was evaluated by the Ftest, testing the significance of b1 and b2. Because secular trends in the management of coronary artery disease might affect death rates, we included the year of death (1986-7, 1988-9, 1990-1, and 1992-3 compared with 1984-5) in the regression models. Pearson correlation coefficients were reported for all comparisons.
During 1984-93 there were 11 010 deaths from coronary heart disease, with average mortality varying from 10.4 deaths per 100 000 population in August to 13.3 per 100 000 in March. Death rates were significantly higher during winter than summer, with the rate in March 22% higher than in August. The average temperature was 25.1°C (range 22.8°C to 27.8°C). Despite the narrow range of temperatures, there was significant annual periodicity with the highest average temperature in August and the lowest in February (figure). The monthly death rate from coronary artery disease and average monthly temperature were inversely correlated (r=−0.55, P<0.001).
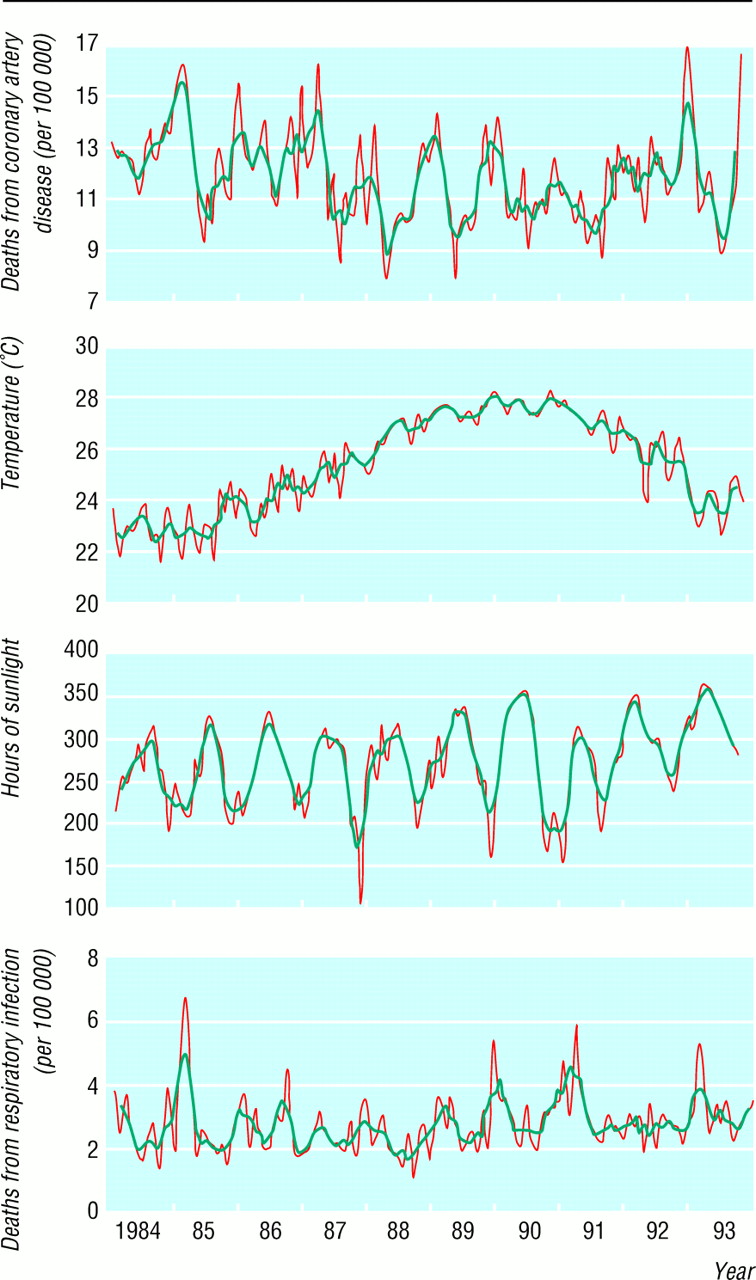
Seasonal variation in death rate from coronary artery disease, average temperature, death rate from respiratory infection, and hours of sunlight by month 1984-93. Grey lines represent monthly rates and black lines three month moving averages. All curves display significant annual periodicity (P<0.001)
{kind=link}
Because sunlight and respiratory infections have been postulated to affect mortality from coronary artery disease we examined the monthly hours of sunlight and mortality from respiratory infection. Both sunlight and mortality from respiratory infection showed annual periodicity (figure). There were 2558 deaths from respiratory infection, with the June rate (2.29/100 000) 33% higher than the February rate (3.4/100 000). The monthly mortality from coronary artery disease was directly associated with the monthly mortality from respiratory infection (r=0.41, P<0.001) and inversely associated with the hours of sunlight per month (r=−0.27, P=0.002).
Comment
We examined the monthly mortality from coronary artery disease in Hawaii, which is closer to the equator than previously studied locations and has a tropical climate with little seasonal variation in temperature. We found a 22% increase in mortality during winter, similar to that noted in Scotland (30%)2 and New Zealand (33%).3
Seasonal variation in mortality from coronary artery disease in Hawaii is consistent with reports of a greater mortality increase with a given fall of temperature in regions with warm winters.1 Our results contrast with a report from New Orleans which noted higher mortality from coronary artery disease during summer than winter.5 Although the relation between coronary artery disease mortality and seasons could be U shaped, with higher mortality associated with extremely hot or cold weather, our data suggest that even relatively small changes in weather may affect mortality.
Acknowledgments
Contributors: TBS conceived the study hypothesis and participated in the study design, data collection, and analysis and writing of the paper. MAM, DAT, RBD, and IK participated in the study design and in the analysis and writing of the paper. TBS is the guarantor.
Funding: None.
Conflict of interest: None.