Article Text

Abstract
OBJECTIVE To examine the influence of socioeconomic deprivation on case fatality following acute myocardial infarction.
DESIGN Prospective cohort observational study.
SETTING General hospital.
PATIENTS 1417 white and south Asian patients admitted with acute myocardial infarction between January 1988 and December 1996, and classified by the Carstairs socioeconomic deprivation score of the enumeration district of residence.
MAIN OUTCOME MEASURES 30 day and one year survival.
RESULTS There was little variation across deprivation groups in age, sex, or smoking status, though a higher proportion of patients from more deprived enumeration districts were diabetic and of south Asian origin, and a higher proportion of them developed Q wave infarction and left ventricular failure. There was no appreciable variation in clinical treatment with deprivation. Patients from more deprived enumeration districts had a higher risk of recurrent ischaemic events (death, recurrent myocardial infarction, or unstable angina) over the first 30 days: event free survival (95% confidence interval (CI)) of the most deprived quartile was 0.79 (95% CI 0.74 to 0.83) compared with 0.85 (95% CI 0.80 to 0.88) in the least deprived quartile. The unadjusted hazard ratio corresponding to an increase from the 5th to 95th centile of the deprivation distribution was 1.54 (95% CI 1.02 to 2.32), and 1.59 (95% CI 1.03 to 2.44) after adjustment for age, sex, racial group, diabetes, acute treatment with thrombolysis and aspirin, and left ventricular failure. Survival from 30 days to one year, however, did not show a socioeconomic gradient (hazard ratio adjusted for the same variables was 1.07 (95% CI 0.68 to 1.70)).
CONCLUSIONS In patients hospitalised with acute myocardial infarction, there is a strong association between early recurrent ischaemic events and socioeconomic deprivation that is not accounted for by clinical presentation or treatment. This association appears to be attenuated over time.
- acute myocardial infarction
- socieconomic deprivation
- survival
Statistics from Altmetric.com
Inequalities in health driven by socioeconomic deprivation continue to undermine the wellbeing of large sections of the population.1 ,2This is particularly true of coronary heart disease, which remains the major cause of premature death in most industrialised countries. Socioeconomic group influences the risk of sustaining a coronary event3-5 and is a major determinant of coronary mortality at the population level.6-10 However, information about the effects of socioeconomic deprivation on case fatality for patients with acute myocardial infarction (AMI) is limited.11
Using education levels as a surrogate for deprivation, North American studies of AMI found a worse prognosis in the least educated people, although whether this reflected differences in health care provision could not be established.12 ,13 In the UK two retrospective studies in Scotland applied Carstairs and Morris deprivation scores to infarct populations but arrived at contradictory conclusions.14 ,15 One of these used the Scottish record linkage system for patients admitted to hospital with AMI and found no indication that socioeconomic deprivation affected case fatality in the first 30 days.14 The other used the Glasgow MONICA (monitoring trends and determinants in cardiovascular disease) coronary event register for patients under 65 and did find a socioeconomic gradient in case fatality that was more pronounced for pre-hospital than for in-hospital deaths.15
In the present study we have re-examined the effects of socioeconomic deprivation on case fatality in a prospective nine year study of patients in a hospital in east London.
Methods
The study was based on patients with AMI admitted to the coronary care unit (CCU) of Newham General Hospital between January 1988 and December 1996 (fig 1). Of the 1616 patients with AMI admitted to the hospital over this period, we excluded from analysis the 61 who were not admitted to CCU and the 39 who were not of white or south Asian background. Of the remaining 1516, we could not classify the deprivation score of 99 patients (see below), leaving a study population of 1417 patients.
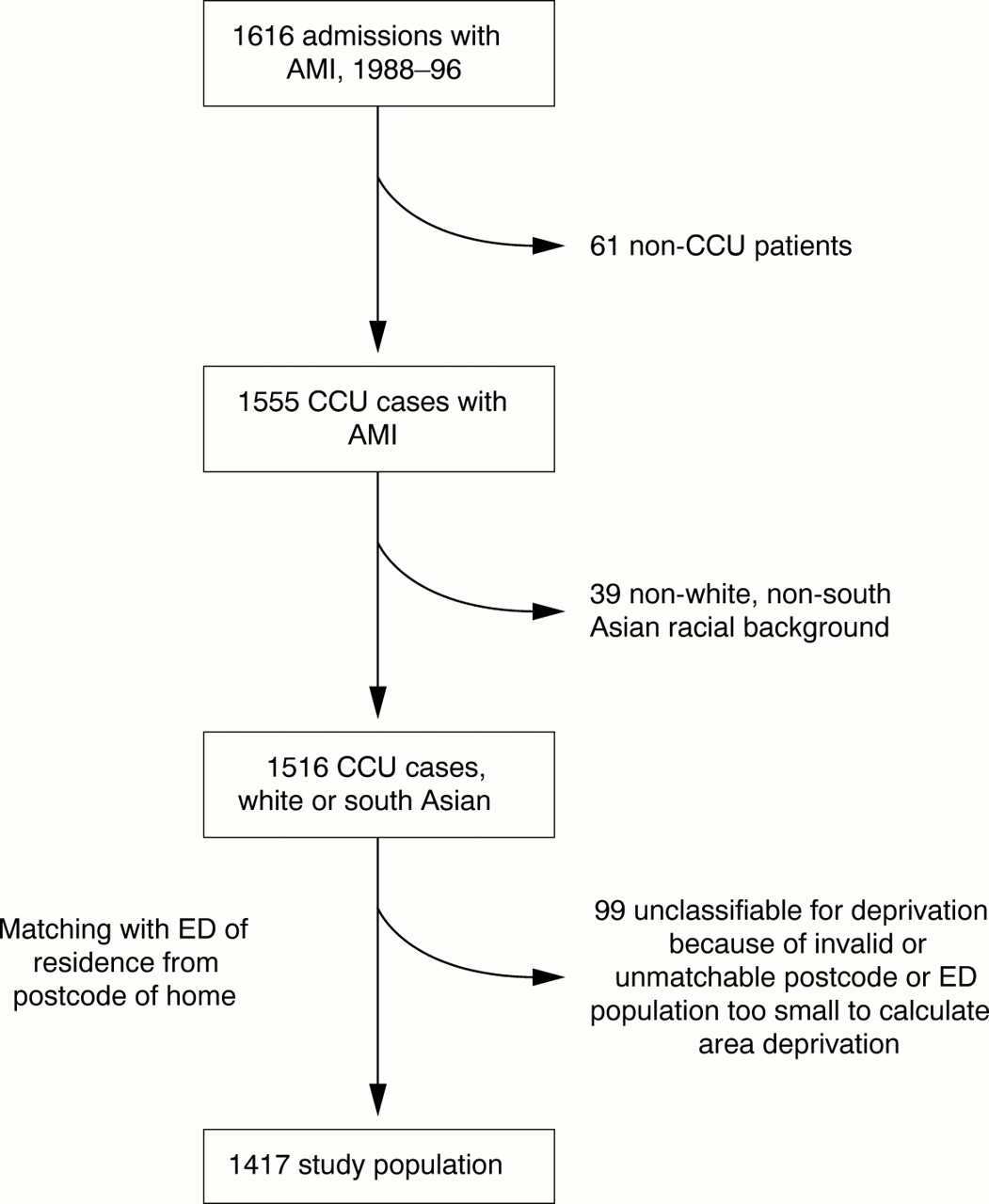
Selection of the study population. AMI, acute myocardial infarction; CCU, coronary care unit; ED, enumeration district.
The diagnosis of myocardial infarction was based on any two of the following three criteria: typical chest pain, > 0.1 mV ST elevation in at least one standard or two precordial leads, and rise in serum creatine kinase to > 400 IU/l (upper limit of reference range is 200 IU/l). Baseline clinical data were collected prospectively and stored electronically as previously described.16 Information recorded included the patient identification number and home address, details of clinical history, examination findings, electrocardiographic data, cardiac enzyme results, and details of treatment in hospital and at discharge. Information regarding race and smoking habit was obtained by direct inquiry. One of three racial groups (white, Asian, or other) was assigned by one of two clinicians (ADT or KR), where necessary by direct inquiry. A diagnosis of diabetes was recorded if the patient required insulin, oral hypoglycaemic drugs, or dietary sugar restriction. The diagnosis of left ventricular failure was recorded for patients requiring diuretic treatment in whom there were radiological signs of interstitial or alveolar pulmonary oedema, or symptoms of breathlessness accompanied by basal crepitations or a third heart sound.
The socioeconomic status of each patient was derived from Carstairs deprivation1 score of his or her enumeration district of residence. (An enumeration district on average contains around 170 households or 400 people.) The Carstairs score, a composite of four census variables—social class of head of household, overcrowding, car ownership, and unemployment—was computed from 1991 census small area data. Patients were linked to the enumeration district of residence by the full unit postcode. Deprivation scores could not be assigned to 99 of the 1516 south Asian and white patients with AMI admitted to CCU because we were unable to match the postcode or because the enumeration district population was too small to calculate an area deprivation score.
Patients were followed up for all cause mortality and recurrent ischaemic events (readmission with unstable angina, AMI, or death) from the admission date until censoring in October 1997. All the patients were flagged by the National Health Service central register to obtain follow up mortality data. For patients in whom information about non-fatal ischaemic events was not already available from outpatient follow up or readmission to hospital, postal questionnaires were used to obtain the information, backed up by telephone inquiry for non-responders. In this way, follow up data beyond discharge were obtained in 98.6% of patients who survived to hospital discharge.
STATISTICAL ANALYSIS
Tables are shown with patients grouped into quartiles of the deprivation distribution. Trends across deprivation groups were evaluated using the non-parametric test described by Cuzick17 and implemented in Stata by thenptrend command. Survival was calculated by the Kaplan-Meier method; survival probabilities are expressed as percentages with 95% confidence intervals (CI). Multivariate predictors of survival are based on a proportional hazard model. Hazard ratios (relative risks) are expressed as the increase in risk corresponding to a change from the 5th to 95th centile of the deprivation distribution. In broad terms, this can be interpreted as the risk of patients from the most deprived enumeration districts compared with that of patients in the least deprived enumeration districts. Significance tests for proportional hazards regression were based on comparisons of likelihood ratios.
Results
CLINICAL CHARACTERISTICS AND TREATMENT
Age and sex distributions were similar for all deprivation groups (table 1). However, the proportion of patients of south Asian origin increased from 15.1% in the least deprived to 46.1% in the most deprived quartile, and the proportion of patients with diabetes from 16.6% to 28.9%. There was no evidence of a significant trend with deprivation in smoking habit, hypertension, or other risk factors.
Patient characteristics, treatment, and clinical complications by quartile (Q1–Q4) of the Carstairs deprivation score
The time from pain onset to hospital arrival was similar for all deprivation groups, as was emergency treatment received in hospital, there being no differences among the groups in proportions receiving aspirin and thrombolysis, or in the time taken to administer thrombolysis.
There were no differences among deprivation groups in infarct location. However, Q wave infarction increased with socioeconomic deprivation, as did left ventricular failure, but not ventricular fibrillation. A suggestive but not significant trend with deprivation was seen in hospital mortality.
Proportions of patients discharged on aspirin and beta-blockers were similar for all groups.
SURVIVAL ANALYSIS
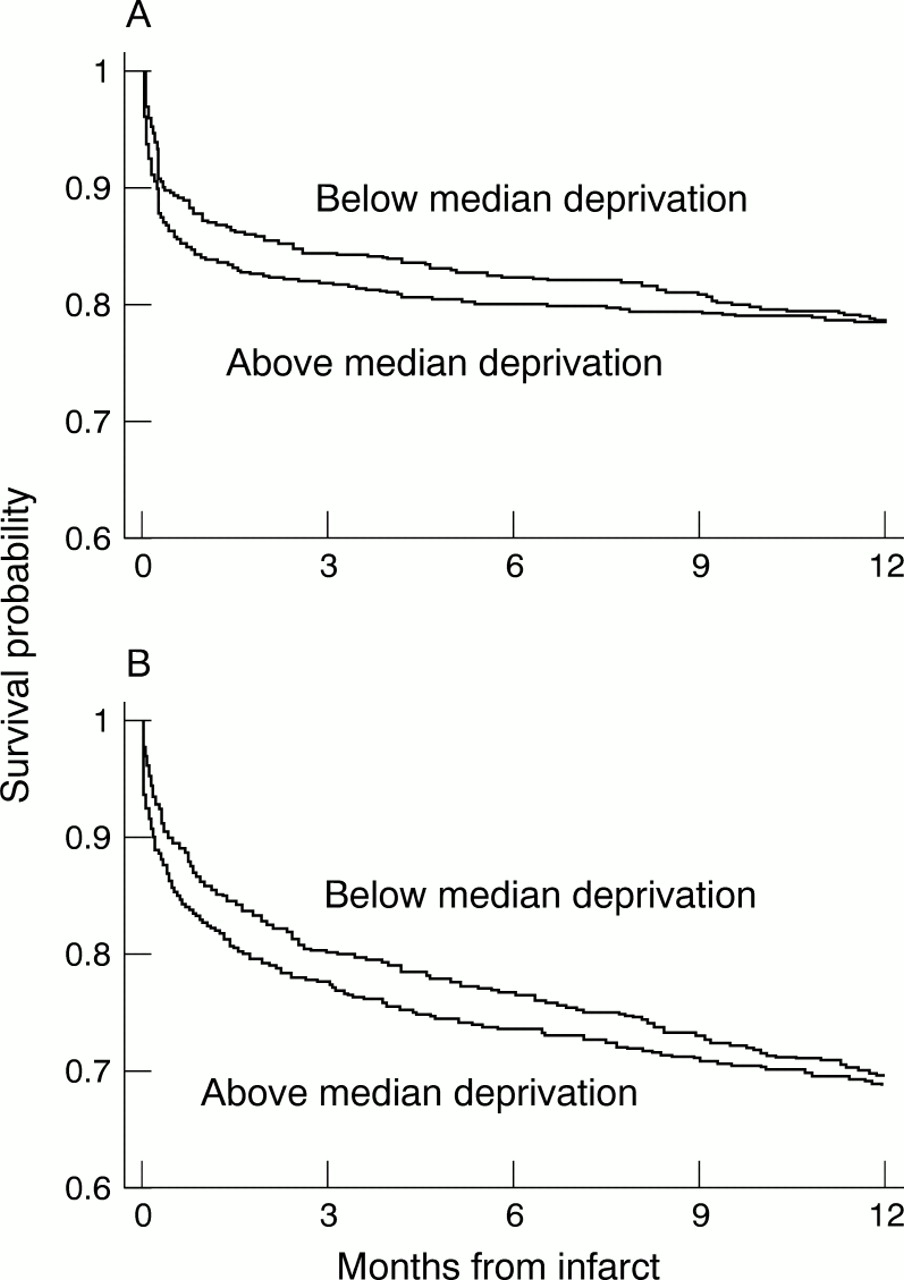
At 30 days, event free survival for both recurrent ischaemic events and mortality fell progressively with deprivation: for recurrent ischaemia from 0.85 (95% CI 0.80 to 88) in the least deprived quartile to 0.79 (95% CI 0.74 to 0.83) in the most deprived quartile, and for mortality from 0.88 (95% CI 0.84 to 0.91) to 0.82 (95% CI 0.77 to 0.85) (table 2). But the deprivation gradient tended to flatten over time (fig 2). Because of the time dependent change in relative risk, we confined further analyses of survival to the first year of follow up, and analysed survival separately over the first 30 days and from day 30 to one year.
Kaplan-Meier event free survival probabilities (95% confidence intervals) by quartile (Q1–Q4) of the Carstairs deprivation score
{kind=link}
{kind=link}
Event free survival by deprivation group: (a) death; (b) recurrent ischaemic event
MULTIVARIATE ANALYSIS
The hazard ratios (corresponding to an increase from the 5th to 95th centile of the deprivation distribution) suggested that patients from more deprived enumeration districts were at significantly greater risk of recurrent ischaemic events over the first 30 days (unadjusted hazard ratio 1.54 (95% CI 1.02 to 2.32) (table 3). Point estimates and confidence intervals were little altered by adjustment for age, sex, racial group, diabetes, acute thrombolytic and aspirin treatment, and left ventricular failure. Significance was lost on additional adjustment for discharge drugs (aspirin and β blockers), though this result was based on the smaller number of patients who survived to discharge and had complete data on discharge medication; in fact the point estimate increased slightly. From 30 days to one year, however, there was no evidence that the frequency of recurrent ischaemic events increased with deprivation, suggesting that the period of increased risk associated with deprivation was short lived. A similar pattern was seen with mortality.
Hazard ratios3-150 (95% confidence intervals) for death and recurrent ischaemic events
Discussion
Our prospective study provides new insights into the relation between socioeconomic deprivation and the short and medium term outcomes of patients admitted to hospital with AMI. The data, which include all age groups, show a clear socioeconomic gradient in recurrent ischaemia and mortality in the first month of AMI, which then appears to be attenuated over time.
This differential in 30 day event free survival is remarkable for two reasons. Firstly, the gradient persisted even after controlling for the main clinical determinants of prognosis,18 ,19 including acute treatment with thrombolysis and aspirin, and left ventricular failure—the single most important predictor of survival over the short and long terms, and a direct marker of myocardial damage. The gradient cannot therefore be readily attributed to differences in known clinical parameters or risk factors.
It is also remarkable because of the comparatively narrow range of socioeconomic deprivation in the local catchment population. The district of Newham, from which our study patients were drawn, is among the most disadvantaged in the country.20 It contains socioeconomically deprived populations but, in national terms, very few from the most affluent part of the socioeconomic distribution (93% of the study patients lie within the most deprived two quartiles of the national distribution). So we were not comparing extremes of affluence and deprivation, but rather the outcome of a patients from across a limited range of socioeconomic status in the lower part of the national distribution.
Similar findings for men hospitalised with AMI have previously been reported by the MONICA investigators, who also drew attention to the overall deprivation of their north Glasgow population.15Taken together, these studies have shown that relatively minor differences in deprivation status, even among populations already skewed towards the lower end of the socioeconomic scale, can have important effects on the early outcome of myocardial infarction.
Although we studied a relatively selective CCU population, this does not diminish the validity of our findings because the adverse effects of deprivation on early survival were unaffected by adjustment for a variety of baseline, clinical, and treatment variables. Moreover, only a small number of all patients admitted to hospital with AMI were not treated in a CCU. Overall, our study population was representative of those in the catchment area, which includes a large south Asian community.18
The use of enumeration district Carstairs scores for classifying socioeconomic deprivation is an established method that, in health analyses, has generally been found to yield socioeconomic differentials of similar magnitude to those based on individual social class.1 The 1991 census from which socioeconomic variables were derived fell in the middle of our study period, 1988 to 1996. In the absence of any more proximate estimates of deprivation at the population level, this ensured that the scores reflected as accurately as possible the deprivation status of our patients at the time they came into hospital.
The mechanisms of the adverse effects of deprivation on the outcome of myocardial infarction are unclear and cannot be clearly deduced from our data. It is reasonable to assume, however, that their major influence was exerted early after coronary occlusion because survival differences among the deprivation groups had largely disappeared by one year. This assumption is supported by the Glasgow MONICA data, which showed that the socioeconomic gradient was more pronounced for pre-hospital deaths than for deaths among patients admitted to hospital.15 It is well established that, in AMI, deaths in the pre-hospital phase are usually arrhythmic while deaths in the hospital phase are usually haemodynamic, caused by extensive myocardial injury.21 ,22 There is unlikely, therefore, to be any simple explanation for the effect of deprivation because it appears to affect both phases of early outcome. Nevertheless, it may be significant that the point estimates of risk for the most deprived group had fallen below those of the least deprived group a year after myocardial infarction, suggesting that some of the excess early risk might reflect a “harvesting” phenomenon related to the impact of myocardial infarction, in addition to the debilitation that commonly accompanies severe deprivation such as nutritional deficiency,23 concomitant illness,24 or autonomic disturbance.25
In conclusion, our findings provide further evidence of the vital interaction between socioeconomic status and health. They make clear that in patients hospitalised with AMI, early case fatality increases with increasing levels of deprivation. Add to this the well established relation between socioeconomic group and the population mortality from coronary heart disease and it is evident that inequalities in health continue to run deep in society. No simple or treatable mechanism is likely to emerge that accounts for the adverse effect of deprivation on coronary mortality, and its resolution in the long term will almost certainly depend on implementation of effective strategies to reduce poverty.