Article Text

Abstract
Purpose Recent epidemiological studies have shown that environmental factors during the fetal period to early childhood might affect the risk of non-communicable diseases in adulthood. This is referred to as the developmental origins of health and disease (DOHaD) concept. The Chiba study of Mother and Children's Health (C-MACH) is a birth cohort study based on the DOHaD hypothesis and involves multiomics analysis. This study aims to explore the effects of genetic and environmental factors—particularly the fetal environment and postbirth living environment—on children's health, and to identify potential biomarkers for these effects.
Participants The C-MACH consists of three hospital-based cohorts. The study participants are pregnant women at <13 weeks gestation. Women who underwent an examination in one of the three hospitals received an explanation of the study. The participants consented to completing questionnaire surveys and the collection and storage of biological and house/environmental samples. Participants were provided unique study numbers. All of the data and biological specimens will be stored in the Chiba University Center for Preventive Medical Sciences and Chiba University Center for Preventive Medical Sciences BioBank, respectively.
Findings to date Consent to participate was obtained from 433 women. Of these women, 376 women completed questionnaires in the early gestational period. The mean age was 32.5 (4.4) years. The mean body mass index (BMI) was 21.1 (3.0) kg/m2. Before pregnancy, 72.3% of the women had a BMI of 18.5–24.9 kg/m2. During early pregnancy, 5.0% of the participants smoked.
Future plans Primary outcomes are allergy, obesity, endocrine and metabolic disorders, and developmental disorders. Genome-level, metabolome-level, umbilical cord DNA methylation (epigenome), gut microbiota and environmental chemical exposure variables will be evaluated. We will analyse the relationships between the outcomes and analytical variables.
- Birth cohort
- Children
- Environmental chemicals
- Pregnant women
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
In the Chiba study of Mother and Children's Health (C-MACH), a wide range of biomaterials such as maternal and child faeces, maternal milk, milk teeth, saliva, umbilical cords and cord blood, etc, from mother–child pairs, are collected.
In the study, environmental factors such as maternal life style and nutritional status, indoor dust and environmental chemicals including in utero exposure are assessed.
In the study, various analytical methods such as genome, DNA methylation analysis, microbiome and metabolome are combined to investigate the health effects of the various environmental factors on children in later life. The children are followed to observe the health effects such as allergies, non-communicable diseases and neurodevelopmental disorders.
This is a hospital-based cohort study. Therefore, the participants might not represent the rest of the Japanese population.
The sample size of the study is relatively small to determine the effects of fetal environmental factors on all health problems of children. Nevertheless, it will provide a foundation for future studies concerning the DOHaD (developmental origin of health and disease) hypothesis.
Introduction
Recent, dramatic changes in social and living environments have led to an increase in allergy-related and lifestyle-related diseases as well as the emergence of mental health issues. Epidemiological research focused on European countries1–3 has shown that the nutritional environment from the fetal period to early childhood might affect the risks of non-communicable diseases (NCDs) in adulthood. This was proposed as the concept of the developmental origins of health and disease (DOHaD).1 ,4 Since then, many studies supporting this theory have been conducted. The idea that the risk of a variety of chronic diseases is affected by prenatal and postnatal environmental factors such as maternal nutrition during the fetal period, lifestyle, stress and exposure to environmental pollutants, in addition to genetic sensitivity, is becoming widely accepted. Therefore, cohort studies are required to elucidate the effects of the fetal environment, including chemical exposure, on postbirth health issues.5
Several mechanisms whereby a child’s early environment might affect their later health have been proposed. One conceivable mechanism is via epigenetic changes to the genome caused by exposure to environmental factors during the fetal period.4
Another theory gaining wide acceptance is that disruption of the gut microbiota balance (dysbiosis) affects the development not only of digestive system-related diseases but also of systemic conditions.6 Because children’s gut microbiota might be affected by that of the mothers,7 there is a need to ascertain the relationships between maternal gut microbiota, children’s gut microbiota, and the risk of subsequent NCDs.
In recent years, metabolomic analysis (the exhaustive analysis of in vivo metabolites) has enabled a more detailed understanding of the changes occurring in vivo. These analyses can now be used to evaluate the effects of environmental factors on health as well as the underlying mechanisms. Several studies using this method are ongoing.8 In one of them, Maitre et al9 reported that urinary metabolites of the first trimester are associated with the birth outcome. Their results indicate the potential of metabolic profiling of urine as a means to identify novel non-invasive biomarkers of risks of a negative birth outcome risk.
Few epidemiological studies have comprehensively used these recently developed, novel analytical techniques—such as transcriptome, epigenome, metabolome or metagenomics—and concepts.7–9 The analyses of epigenetic changes, gut microbiota and the metabolome in epidemiological research, might identify new biomarkers for predicting disease risk and determining the effects of environmental factors at an early stage. To improve public health in the 21st century, it is necessary to discover next-generation, preventive intervention techniques during the fetal period that will help to lower the risk of chronic disease.
From this perspective, the Chiba study of Mother and Children's Health (C-MACH) should be regarded as a birth cohort study using ‘omics’ analysis, including genome analysis. C-MACH is a cohort study that began in 2014 and is currently underway. The study consists of three hospital-based cohorts from Onodera Ladies Clinic and Yamaguchi Women's Hospital, both in Chiba Prefecture, and Aiwa Hospital in Saitama Prefecture. Chiba and Saitama are both prefectures adjoining Tokyo, Japan’s largest city, with populations of about 6 200 000 and 7 240 000, respectively.
Study participants are residents of Chiba or Saitama prefecture who underwent normal monitoring during pregnancy. This study aims to explore the effects of genetic and environmental factors, particularly the fetal environment and postbirth living environment, on children’s health, and to identify biomarkers for these effects.
This prospective cohort study, potentially continuing for a decade, will constitute a current and future resource. Our objective is for C-MACH to provide a broad-based platform for both, present research topics and those that will emerge in the future. The following are our specific, approved research objectives:
Ascertain the links between nutritional intake by pregnant women, and fetal development.
Establish biomarkers and indicators of epigenetic alteration to predict children's health problems, such as obesity, allergies and impaired mental development.
Explore whether the interaction between fetal/neonatal environmental factors and genotypes is associated with mental development during childhood.
Explore whether the gut microbiota of mothers affects the development and health of their children, and clarify the factors that affect post-birth changes in gut microbiota.
Ascertain the effects of fetal exposure to environmental chemicals on epigenetic changes and the blood metabolome in children.
Cohort description
Eligibility and exclusion criteria
The study participants at enrolment were pregnant women at <13 weeks gestation. The recruitment population consisted of all pregnant women examined at <13 weeks gestation in the three hospitals. In the event of a stillbirth, participation in this cohort will cease for the mother.
The recruitment population also consists of all children born to women who consented to participate. If a woman withdraws from participation herself, her child or children will also be withdrawn. The fathers of all recruited children were also candidates for participation. Fathers received an explanation of the study, and their consent was obtained simultaneously with that of the mothers. Participating women will be withdrawn from the study if they are transferred to a different hospital for any reason.
Sample size
The target sample size was 500 pregnant women and 500 fathers. The target sample sizes for the umbilical epigenome study and gut microbiota analysis were 500 and 100 pregnant women, respectively.
This cohort study aims to evaluate the influences of fetal environment and postbirth living environment on children's health and diseases. In Japan, the prevalence of childhood obesity is approximately 10%,10 and the prevalence of developmental disorders, including mild disorders, is approximately 8–9%. Based on the outcome of obesity, we designed the study to have 90% power to detect a 1 kg/m2 difference10 between the high and low-exposure groups. The resulting estimated sample size was approximately 380 participants. In addition, we used the Japanese version of the Modified Checklist for Autism in Toddlers (M-CHAT) to screen for the risk of developmental disorders.11 We designed the study to have 90% power to detect a 0.5-point difference between the high and low-exposure groups. The resulting estimated sample size was approximately 330 participants. To estimate the sample sizes, we used the statistical programme R V.3.2.0 ( http://cran.ism.ac.jp). We think that the selected sample size enables evaluation of the effects of the fetal environment on health issues such as obesity and developmental disorders.
To explore biomarkers and indicators of epigenetic or metabolomic alterations associated with children's health problems, multivariate analysis will be performed. The sample size needs to be several hundred participants in order to generate statistically valid results.9 Although several hundred participants are also required for metagenomic analysis, we only collected faeces samples from a hundred mother-child pairs. This part of the study may be underpowered to have definite results.
Recruitment
Recruitment began in February 2014 and ended in June 2015. The numbers of births at each hospital in 2014 were 1786 at Yamaguchi Women’s Hospital, 344 at Onodera Ladies Clinic and 2746 at Aiwa Hospital; the percentages of pregnant women who underwent their initial examination at <13 weeks gestation were 76%, 90% and 100%, respectively. Therefore, there were approximately 4000 potential candidates. Only women who were due to give birth at the participating hospitals were included in the study population.
Information about the study was disseminated on notice boards inside the hospitals and on our website (http://cpms.chiba-u.jp/kids/). At each hospital, the information was provided by a research coordinator or a doctor. If a pregnant woman requested information at a hospital, the staff member responsible was contacted by telephone to provide additional information. If the woman agreed to participate, her written consent was requested and collected. Consent included completing the questionnaire surveys and agreeing to the collection, storage and analyses of biological and house-environmental samples. The participants are able to withdraw from the study at any time.
Informed consent was obtained from the participating mothers on behalf of their children. Children only became participants when consent was obtained from their mothers. The partners of participating women became candidates for participation when the women signed the consent form. The study was explained to the partners when obtaining informed consent from the women. If the partners consented, they also provided informed, written consent to participate.
Language was not an issue because almost all residents of Japan are Japanese citizens. Therefore, the information sheet and other documents were only written in Japanese.
Follow-up programme
All participants will be followed until the child reaches the age of 5 years. The follow-up schedule is shown in figure 1. Follow-up will be completed mainly via questionnaire. The items to be investigated at each stage are described in detail in the following paragraphs.

Follow-up programme. *Continued follow-up after the age of 5 years will be considered later.
Data obtained from regular pregnancy check-ups will be collected until birth. During the first and last trimesters, questionnaires will be administered, and blood, urine and faeces samples will be collected. The questionnaire items include socioeconomic status, lifestyle habits, Brief Diet History Questionnaire (BDHQ) and psychological assessment.
The usual medical findings will be anthropometrically recorded at birth. Umbilical cords will be collected from each hospital. Umbilical cord blood, placenta and faeces samples will be collected from the Onodera Cohort. After birth, questionnaires will be administered to the mothers, and blood, urine and breast milk samples will be collected to analyse environmental chemical, hormone, immunoglobulin (Ig) E and cytokine levels. Video footage of the Yamaguchi Cohort will be recorded to measure the general movement of the children.
Data for the children will subsequently be collected from health check-up records and questionnaires about child development and disease history at the age of 1, 4, 10 months, 1.5, 3.5 and 5 years. Gaze measurement will be completed at the age of 10 months and 1.5 years, as a possible diagnostic index for autism spectrum disorders. The M-CHAT will be performed at the age of 10 months and 1.5 years. Blood samples will be collected from children at the age of 3.5 years. Blood sampling and other invasive tests with the children will be completed so as to minimise the burden on them.
The collected samples will be stored at −80°C in the Chiba University Center for Preventive Medical Sciences (CPMS) BioBank. They will be preserved as biological specimens until the analysis is completed.
Outcome measurements
Primary outcomes are allergies, obesity, endocrine and metabolic disorders and developmental disorders. These data will be obtained using the questionnaires. Other outcomes are perinatal complications, congenital deformities and neuropsychological impairment. To assess obesity in the children, the body mass index (BMI) will be calculated using height and weight extracted from the follow-up data. The children's allergy status will be assessed using serum IgE levels for some allergens. M-CHAT and gaze measurement at the age of 10 months and 1.5 years will be performed for the outcome of developmental disorders. Perinatal complications, congenital deformities and neuropsychological impairment will be extracted from the questionnaires, and from the mother and child health notebooks.
Evaluated variables
Genome-level, metabolome-level, umbilical cord DNA methylation (epigenome) and gut microbiota variables will be analysed (table 1). An overall assessment of these results will be considered with the environmental factors and childrens’ health outcomes. In addition to maternal and child metabolomic analysis, gut microbiota and umbilical cord DNA methylation, umbilical cord blood cytokine concentration measurements and analysis will also be conducted to help identify biomarkers.
Target field, analysis and materials
Questionnaires
Several questionnaires will be administered at several time points. We will assess the health status of the mothers and children, using questionnaires. The self-administered BDHQ will be used to assess the general maternal nutritional status. Other questionnaires will be administered for the following items: educational background, occupation, income, smoking habit, including passive smoking, and alcohol consumption during pregnancy.
Exposure assessment
As already described, this study will investigate the effects of exposure to environmental chemicals. In the study, polychlorinated biphenyl (PCB) levels in maternal and umbilical cord blood will be measured as an index of the exposure to persistent organic pollutants (POPs). We previously reported that PCB concentrations in blood and umbilical cord samples are correlated with the concentrations of various POPs.12–17 To assess the effects of the indoor environment, indoor dust samples will be collected and measured for house dust, mites, mould and endotoxins.
PCB levels will be measured using gas chromatography–mass spectrometry.18 ,19 In addition to total concentration, the composition of major individual congeners will also be analysed and the source of exposure inferred. The associations between congener composition and outcomes will also be analysed.
Genomic analysis
Genomic analysis will be conducted with maternal blood samples, and saliva samples from the children and partners. DNA will be extracted, and genome-wide association analysis using single-nucleotide polymorphisms will be conducted to examine the genomic effects on outcomes, such as allergies.
Epigenetic analysis
DNA methylation is one of the mechanisms hypothesised in the DOHaD model.20 Comprehensive epigenetic analysis will be performed to investigate DNA methylation in the umbilical cord,21 using a microarray (Illumina iScan System and Infinium HumanMethylation450 BeadChip, Illumina, San Diego, California, USA) and methylation-sensitive high-resolution melting (HRM) analysis. We will examine the variation of DNA methylation of umbilical cords, using a DNA methylation array. We will extract the area/s that is/are correlated with outcomes. The detected candidate areas will be examined using HRM for all umbilical cord samples.
Metagenomic analysis
Metagenomic analyses will be conducted. Gut microbiota will be analysed using 16S rRNA sequences.22 Gut microbiota DNA will be extracted from stool samples collected from mothers and their children; 16S rRNA sequence data will be obtained, and the distribution and bias of gut microbiota will be analysed.
Metabolomic analysis
High-performance liquid chromatography/tandem mass spectrometry will be used to perform semiquantitative targeted metabolome analysis of umbilical cord blood and mother's urine.23 The composition of metabolites, such as amino acids, lipid metabolites, and vitamins in blood and urine, and their associations with outcomes, such as obesity or developmental disorders, will be analysed. Some biomarkers for obesity and autism spectrum disorders were found in previous studies.24 ,25 Most metabolomics studies use a non-targeted qualitative approach; however, targeted metabolome analysis might be useful for epidemiological studies, due to their accuracy and quantitative nature. A search for biomarkers, using a semiquantitative approach, will be conducted, and the mechanisms for changes in metabolomes will be examined.
Covariates and potential confounders
Socioeconomic status, lifestyle habits, nutritional habits and physical environment will also be investigated as covariates and confounders. These data will be obtained from questionnaires. Biochemical tests and hormone-level measurements will be completed with maternal and umbilical cord blood. Cholesterol, glycoalbumin and some vitamins will be measured using maternal blood during the first and third trimester, and cord blood. Hormones such as cortisol, oestrogen and oxytocin will be measured using saliva of children at the ages of 10 months and 1.5 years (figure 1). We will store these samples as necessary.
Statistical analysis
Data are and will be reported as mean (SD). Bivariate analyses will be conducted to determine the correlations between the dependent variables, such as BMI, M-CHAT and serum IgE levels, and independent variables. In addition, a hierarchical Bayes model, l1/l2 regularised regression analysis, random forest, gradient boosting decision tree and/or projections to latent structures analysis, adjusted for potential confounding variables, will be conducted to estimate the relative risk of incident obesity, an M-CHAT score above the cut-off point, or a serum IgE level above the cut-off point. DNA methylation levels will be treated as both, dependent and independent factors. The correlation between DNA methylation levels and fetal environmental factors will be analysed as dependent factors. The DNA methylation levels will be treated as independent factors in the analyses for the outcomes. Statistical significance is set at p<0.05 for all analyses. In addition, microarray or microbiome data will be analysed using a false discovery rate.
Data management system and biospecimen storage
Participants have been assigned unique study numbers. All of the data will be stored in the Chiba University CPMS. Blood, umbilical cord, umbilical cord blood, placenta, breast milk and stool samples will be stored at −80°C in the Chiba University CPMS BioBank until testing.
Ethics and dissemination
The study protocol was approved by the Biomedical Research Ethics Committee of the Graduate School of Medicine, Chiba University (ID 451: application date 8 November 2013; ID 462: application date 4 December 2013; ID 502: application date 28 May 2014). Informed consent was obtained from the study participants.
Study results will be disseminated at national and international conferences. The results will be provided to the public by publication in academic journals. We also intend to disseminate our results to the public on our web site.
Findings to date
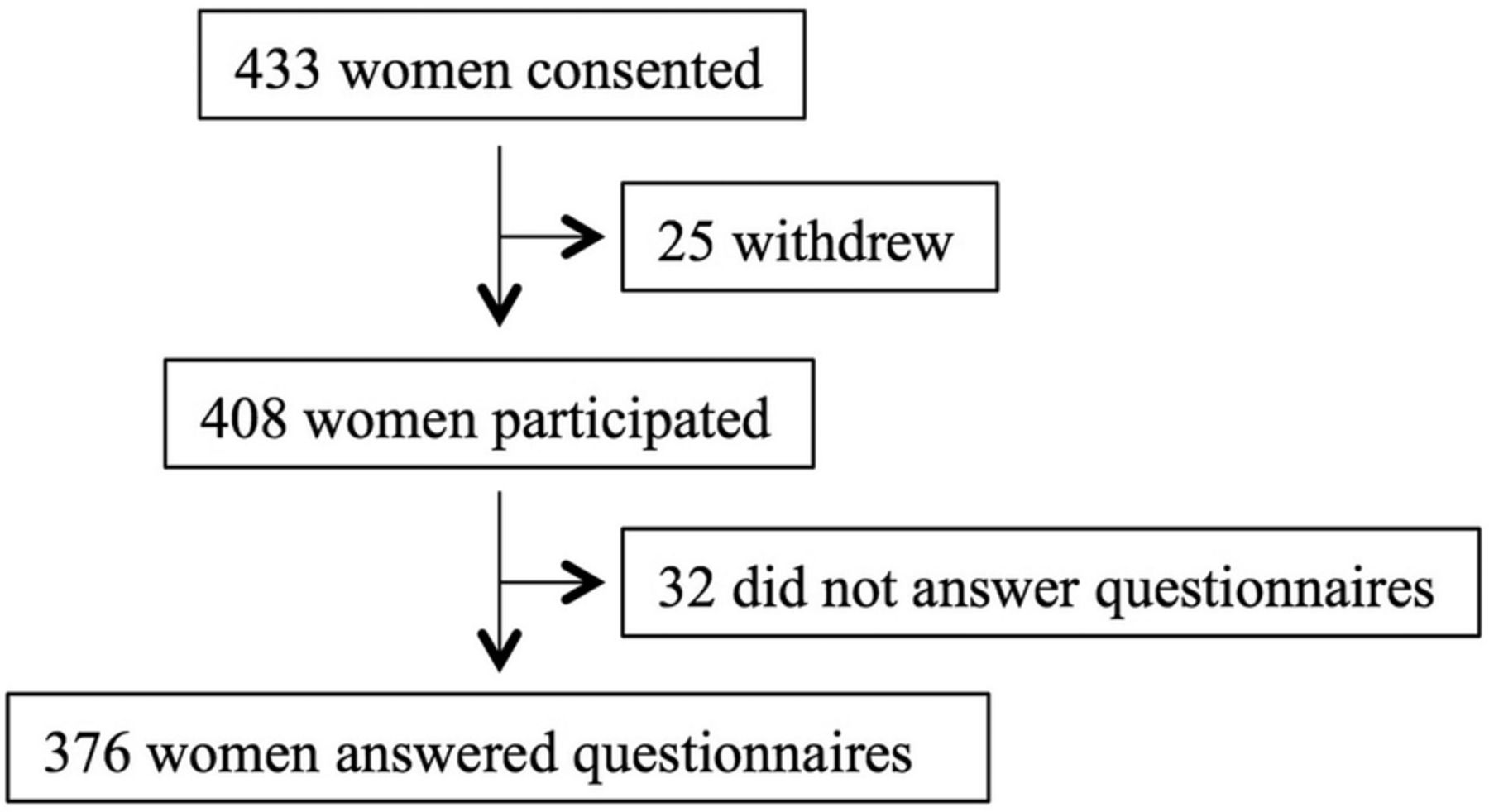
Consent to participate in C-MACH was obtained from 433 women. Twenty-five women withdrew after providing informed consent, resulting in a final cohort of 408 women. Of these 408 participants, 32 women did not complete the baseline questionnaires (figure 2). Therefore, we collected questionnaires from 376 women in the early gestational period. These participants were almost 10% of the potential candidates. We randomly contacted approximately one-fifth of all the participants who came to the hospitals and clinics. Around half of them consented to the study.

{kind=link}
{kind=link}
Flow diagram of study participants.
Of the 376 women, 5.1% were ≤24 years old, 19.4% were 25–29 years old, 41.7% were 30–34 years old and 33.8% were ≥35 years old. The mean age was 32.5 (4.4) years. The mean age of women expecting their first child was 31.8 (4.2) years. This was older than the mean age obtained from Japanese population data (29.7 years).26 As shown in table 2, the majority of the women were married and had an appropriate pre-pregnancy BMI (18.5–24.9 kg/m2; 72.3%), similar to other Japanese cohort studies.27 Smokers during early pregnancy accounted for 5.0% of the participants, which is lower than the percentage in other Japanese cohort studies.27–29
Maternal characteristics
Strengths and limitations
A strength of this study is the combination of a variety of analyses to investigate the effects of the various factors on children. The results of this study will provide a foundation for future studies concerning the DOHaD hypothesis, as well as other large-scale cohort studies. We anticipate that it will provide new information for studies in the areas of genomics, epigenomics, metagenomics and metabolomics.
Our study will provide a comprehensive evaluation of in utero environmental factors by assessing the effects of pollutant exposure, maternal gut microbiota and the external environment on the fetus, in addition to evaluating variables related to maternal lifestyle, nutrition and blood biochemistry.
This study is a prospective cohort study designed to collect data on a variety of environmental factors, including in utero exposure to chemicals. Detailed data are required to detect the latent effects of environmental factors during the fetal and neonatal periods on outcomes during childhood.
We will publish regular bulletins and send them to participants to encourage their continued participation in the study.
The sample size is not large enough to determine the effects of fetal environmental factors on asthma, atopic dermatitis, diabetes and neurodevelopmental disorders. This study will follow children until they are 5 years old. This duration might not be long enough to fully evaluate the DOHaD hypothesis. Therefore, continued follow-up after the age of 5 years will be considered later.
Because this is a hospital-based cohort study, the participants might not be representative of the rest of the Japanese population. We could not contact all potential candidates because of the limited number of staff members. We could contact one-fifth of potential candidates, although the ratio of contacted participants to all potential candidates was slightly different for each medical institution. Therefore, sampling bias might be present. Another limitation of this study is a potential change in residence by the participants.
Collaboration
The C-MACH is open to future joint studies with external study groups. Researchers can submit a joint study proposal to the C-MACH research committee. The group will consider these proposals and determine if they will be adopted. The screening criteria will include whether the proposed study protocol (1) is in accordance with the C-MACH objectives, (2) does not overlap with other studies already underway, (3) has the funding available to proceed and (4) does not disadvantage the cohort participants. The call for joint study proposals from external groups will open after recruitment is complete, the basic data set has been confirmed, data cleaning is concluded and the initial results have been confirmed.
Acknowledgments
The authors would like to acknowledge the C-MACH participants and staff for their dedication.
References
Footnotes
Collaborators Chiba study of Mother and Children's Health (C-MACH) Group: Chisato Mori; Akira Hata; Emiko Todaka; Akihiro Sekine; Shinsuke Fujita; Naoki Shimojo; Kenichi Sakurai; Yoshiharu Matsuno; Masamichi Hanazato; Kaori Tachibana; Hiroko Nakaoka; Midori Yamamoto; Hidenobu Miyaso; Masae Otake; Norimichi Suzuki; Masahiro Watanabe; Hisao Osada; Satomi Shiga; Akiko Kawanami; Shunya Takase; Chie Koga; Hideoki Fukuoka; Kiminori Nakamura; Kazuyuki Shinohara; Masaki Kakeyama; Hirokazu Doi; Erika Sawano; Toshio Tsuji; Zu Soh; Koji Shimatani; Satoru Yamaguchi; Tsutomu Onodera; Takuhiro Yamada.
Contributors The authors are justifiably credited with authorship, according to the authorship criteria. CM is the primary investigator of this study. CM, ET and AH conceived the study idea and designed the study. YM, HM and MY performed the administrative procedures. HF supervised the study design and protocol development. KS and CM supervised the study from the medical and clinical aspects. AE and CM supervised the study from the exposure science aspect. KS wrote the draft and edited the manuscript. All the authors participated in the discussion of the protocol development and revision of the manuscript.
Funding This research was supported by JSPS KAKENHI Grant Number 20241016 and 15H06087 and grants from the Chiba Foundation for Health Promotion & Disease Prevention.
Competing interests None declared.
Ethics approval the Biomedical Research Ethics Committee of the Graduate School of Medicine, Chiba University.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement The C-MACH is open to future joint studies with external study groups. Researchers can submit a joint study proposal to the C-MACH research committee. The group will consider these proposals and determine if they will be adopted. The screening criteria will include whether the proposed study protocol (1) is in accordance with the C-MACH objectives, (2) does not overlap with other studies already underway, (3) has the funding available to proceed, and (4) does not disadvantage the cohort participants. The call for joint study proposals from external groups will open after recruitment is complete, the basic data set has been confirmed, data cleaning is concluded and the initial results have been confirmed.