Article Text

Abstract
Aims: To determine whether an increase in effort-reward imbalance over time increases the risk of angina, and whether such increases are associated with lower occupational position.
Methods: Effort-reward imbalance (ERI) at work was measured in the Whitehall II occupational cohort of London based civil servants at baseline (1985–88) and in 1997. Coronary heart disease was measured in a self-reported health questionnaire by combining the Rose Angina Questionnaire with doctor diagnosed angina in 2001.
Results: Among men, increase in ERI over time was associated with an increased risk of incident angina. Moreover, as increases in ERI were more common among lower grade civil servants, change in imbalance, to some extent, contributed to explaining the social gradient in angina. Among women, increases in imbalance were not associated with risk of angina, and therefore did not contribute to the explanation of the social gradient.
Conclusions: Reductions in effort-reward imbalance at work may reduce the risk of coronary heart disease among men.
- CHD, coronary heart disease
- ERI, effort-reward imbalance
- effort-reward imbalance
- angina
- social gradient
- pathways
Statistics from Altmetric.com
There is considerable evidence of a social gradient in coronary heart disease (CHD)—people from more disadvantaged groups and classes have higher risks of CHD.1,2 Adverse psychosocial work environments have been hypothesised to have detrimental long term effects on the cardiovascular system.2,3 Furthermore, there is some evidence that such adverse psychosocial work environments are more frequent among more disadvantaged groups and that this may contribute to the explanation of the social gradient in CHD.4
Two theoretical models of adverse psychosocial work environments have been proposed and tested in prospective investigations of cardiovascular epidemiology: the demand control model5 and the effort-reward imbalance model.6 The former model puts emphasis on distinct characteristics of the workplace: job task profiles defined by high quantitative demands and a low degree of decision latitude or task control are assumed to elicit sustained stress reactions with adverse long term effects on the cardiovascular system. A majority of studies support this model in terms of predicting CHD.2,3,7,8 The more recently developed effort-reward imbalance model is based on the norm of reciprocity of work contracts. Effort at work is reciprocated by socially defined rewards that include money, esteem, and status in terms of promotions prospects and job security. However, an imbalance between (high) efforts spent and (low) rewards received in turn, is likely to be experienced by employed people under the following conditions: (1) if employees have little choice of alternative workplaces (for example, due to low level of skill or a critical business cycle); (2) if employees accept this imbalance for strategic reasons (that is, to improve their future chances by anticipatory investments); (3) if employees exhibit a specific psychological pattern of coping with work demands characterised by excessive commitment (work related over-commitment). The effort-reward imbalance model, too, has been successfully tested in several prospective epidemiological investigations, and has been shown to produce an effect size similar to the one produced by the demand control model, thus indicating a complementary role of the two models of adverse psychosocial working environments.2,3,8,9
So far, there has been little research on the health effects produced by changes in the effort-reward imbalance at work over time. In particular, does an increase in the imbalance result in an increased risk of CHD, even after adjusting for the initial level of effort-reward imbalance? An answer to this question seems crucial in view of increasing economic competition, in combination with reduced rewards (in terms of restricted salaries, reduced promotion prospects, and increased job insecurities experienced) by more and more people in a globalised economy.10
The Whitehall II study is a prospective investigation of socioeconomic, psychosocial, behavioural, and biomedical health determinants in a cohort of British civil servants.11 Previous analyses have shown that employees from lower employment grades and with greater effort-reward imbalance from the first phase (1985–97) of the Whitehall II study have higher risks of incident CHD after 10 years (by the fifth phase of the study, 1997).9 This paper proposes to extend this analysis further in two ways—by looking at new CHD (self-reported) health outcomes after the fifth phase, and by analysing the change in employees’ effort reward imbalance from phase 1 to phase 5, to see whether this predicts incident CHD by 2001. As the latest phase of the Whitehall II study for which data are available (phase 6) is a questionnaire phase, incident CHD could only be examined in terms of self-reported doctor diagnosed angina or the Rose Angina Questionnaire.
The relation between effort-reward imbalance and socioeconomic position has been found to be inconsistent. This is mainly due to the fact that the mean level of effort increases with higher socioeconomic position, whereas the mean level of reward decreases with lower socioeconomic position.12 Although there are exceptions in specific occupational groups and although results may vary according to the operational definition of effort-reward imbalance, this general trend results in an inconsistency of the association of imbalance with socioeconomic status. In some studies, an inverse social gradient of the ratio was documented,13,14 while in at least two reports an opposite trend was obvious.9,15 However, none of the studies measuring work stress by this model used repeated measures of effort-reward imbalance. It is possible that change in the level of work stress over time is associated with socioeconomic status, leaving those in lower positions with a lower chance of reducing their effort-reward imbalance at work.
Main messages
-
Increased effort-reward imbalance at work among men is associated with increased risks of angina among men.
-
Those in higher occupational classes are more likely to reduce their exposure to effort-reward imbalance at work over time compared to those in lower occupational classes.
This paper sets out to test the following interrelated hypotheses in the frame of a prospective epidemiological investigation, the Whitehall II study:
-
Is there a social gradient of angina incidence, as measured by occupational class?
-
Is effort-reward imbalance at work, as assessed at study onset, associated with an increased risk of angina, even after adjusting for the social gradient?
-
Does an increase in effort-reward imbalance over time increase the risk of angina, even after adjusting for initial level of effort-reward imbalance?
-
Does occupational class predict changes in effort-reward imbalance? Do higher grade employees decrease and lower grade employees increase or maintain their effort-reward imbalance over time?
Hypotheses 1 and 2 have been examined before in other studies, including the Whitehall II study. Hypotheses 3 and 4 are new hypotheses that have not been examined in previous studies, to the authors’ best knowledge.
METHODS
Data
The Whitehall II study is a prospective investigation of socioeconomic, psychosocial, behavioural, and biomedical health determinants in a cohort of 10 368 male and female British civil servants.11 Data collection started in 1985–88 (phase 1) and was continued to 2001 (phase 6). At phase 6, data were available from 7344 participants, but for some variables such as work conditions, the effective sample size was much smaller as the analysis was restricted to those who were still in employment at phase 5. Of the 5002 respondents who were in employment at phase 5, 3697 answered all the questions on the effort-reward imbalance questionnaire. Respondents who were still in employment at phase 5 but did not answer all the questions on the effort-reward imbalance questionnaire were older and from lower employment grades.
Measures
Angina is the most frequent manifestation of CHD and the most important precursor of acute myocardial infarction.15 Angina at phase 6 was measured by the Rose Angina Questionnaire16 or by available information on (self-reported) doctor diagnosed angina. New cases of self-reported angina from phase 5 (1997–99) to phase 6 (excluding prior CHD up to and including phase 5) were considered. As mentioned, an earlier report from the Whitehall II study has already published evidence on the effect of effort-reward imbalance on CHD from phase 1 to phase 5. This paper builds on the results from the previous study by examining incident angina beyond that study period, as well as by considering change in effort-reward imbalance from phases 1 to 5.9 Around 3% of the effective sample who had never had a CHD event (139 men, 67 women) reported new cases at phase 6. In prior studies, this measure of angina was shown to be a reliable marker of clinically expressed CHD.17
Policy implications
-
Reductions in effort-reward imbalance at work may reduce the incidence of heart disease among men.
-
The design and implementation of theory based intervention measures on reducing adverse psychosocial work conditions is indicated.
Effort-reward imbalance at work: The model of effort-reward imbalance at work was measured, at phase 5, by a psychometrically validated questionnaire containing 23 Likert scaled items.12 This questionnaire contains three scales: a scale measuring effort at work (6 items), a scale measuring reward at work (11 items, composed of three subscales: “esteem”, “salary and promotion”, “job security”), and a scale measuring the personal pattern of coping with work demands, “over-commitment” (6 items). The first two scales measure the extrinsic component of the model (perceived demands and rewards at work), whereas the third scale measures the intrinsic component of the model (the psychological coping pattern). The central hypothesis of the model assumes a linear association of effort-reward imbalance with health: the higher the imbalance the higher the health risk. To estimate this imbalance, a ratio of the two scales “effort” (e) and “reward” (r) is constructed according to the formula e/r · c, where c is a correction factor for unequal number of items in the enumerator and denominator.
The English version of the questionnaire measuring the full effort-reward imbalance model (extrinsic and intrinsic component) was applied at phase 5, but was not available at phase 1. Therefore, a proxy measure was constructed based on a broad range of questionnaire items measured at phase 1 that relate to an adverse psychosocial environment. This proxy measure was restricted to the two scales, “effort and reward”, representing the extrinsic component of the model. The construction of this measure has been described elsewhere, and was successfully tested with regard to the prediction of incident CHD events in the Whitehall II study.9
As effort-reward imbalance was measured by non-identical instruments at phases 1 and 5, convergent validity analyses were examined to see if the associations of both measures with age, self-rated health, and job strain18 were similar. Previous analysis has shown that effort-reward imbalance decreases with age9,12,13 and is associated with poorer self-rated health.19–21 Both measures of effort-reward imbalance (at phases 1 and 5) showed similar associations with age and self-rated health. Furthermore, the correlations between job strain (that is, high demands and low control) and effort-reward imbalance at both time points were remarkably similar: 0.40 at phase 1 and 0.42 at phase 5. This suggests that the measures of effort-reward imbalance at both time points are comparable.
Change in the effort-reward imbalance ratio was measured by subtracting the phase 5 score from the phase 1 score. Thus, a higher value of the difference score implies a greater reduction in the effort-reward imbalance from phase 1 to 5, and vice versa. This score was tertiled for some of the descriptive analyses: effort-reward imbalance increased, remained the same, and decreased (although these titles do not strictly describe the groups as very few respondents reported higher imbalance at phase 5 compared to phase 1).
Occupational class was measured by the hierarchical measure of civil employment grade, distinguishing six grades from highest (permanent secretary) to lowest (administrative officer, assistant) occupational positions.11 For ease of presentation for the figures, this variable was recoded into three groups—high, middle, and low grades.
Risk factors for phase 6 angina (obesity—measured by the body mass index, and systolic blood pressure) were measured at phase 5. Other cardiovascular risk factors were also examined (diabetes, diastolic blood pressure, smoking, and physical activity), but these were not significantly related to incident angina from phase 5–6, and so were dropped from the analyses.
Statistical analysis
Pathway models were analysed to examine the inter-related hypotheses. Figure 1 shows the basic figure for these models. In fig 1, path A denotes the correlation between employment grade at phase 1 with effort-reward imbalance at phase 1. Path B denotes the effect of employment grade on imbalance at phase 5. Path C examines the effect of imbalance at phase 1 on imbalance at phase 5. Path D denotes the effect of imbalance at phase 5 on angina at phase 6. Path E denotes the direct effect of imbalance at phase 1 on angina. Path F denotes the direct effect of employment grade on angina. As these pathways are estimated in the same model (that is, adjusted for each other):

Path diagram showing associations between employment grade, effort-reward imbalance at two time points, and angina.
-
Evidence for path B would suggest that employment grade affects change in effort-reward imbalance (or the variance in effort-reward imbalance at phase 5 that is unexplained by imbalance at phase 1)
-
Evidence for path D would suggest that change in effort-reward imbalance (or imbalance at phase 5 adjusted for imbalance at phase 1) affects angina.
This basic pathway model was expanded to include age (at phase 1), obesity (at phase 6), and blood pressure (at phase 6). Age was correlated with the phase 1 variables (employment grade and effort-reward imbalance) and affected effort-reward imbalance at phase 5 and angina at phase 6. Obesity and blood pressure (measured at phase 5) affected angina at phase 6 and were correlated with the other variables in the model. To examine this pathway model, MPlus software was used which enables path analysis with categorical outcome data. The pathways were analysed using weighted least squares probit regressions, rather than maximum likelihood logistic regressions. In order to handle patterns of missingness in the data, (including drop out from the study at phase 6 as well as missing effort-reward imbalance data at phase 5), MPlus provides maximum likelihood estimation under MCAR (missing completely at random) and MAR (missing at random) assumptions. In the analysis, missingness is allowed to be a function of the observed covariates, age and employment grade, as older respondents and those from lower grades were more likely to be missing at phase 6 as well as have missing effort-reward imbalance data at phase 5. The outcomes (including missing data) are modelled conditional on the covariates and the covariates have no distributional assumption.
RESULTS
In table 1, the percentage of new cases of angina is given by employment grade (at phase 1), tertiles of effort-reward imbalance at phases 1 and 5, and the difference score between the two (separately for men and women). There were 206 cases of incident angina (139 men, 69 women). Although 3697 respondents filled in the effort-reward imbalance questions at phase 5, not all of them were followed up at phase 6, resulting in the smaller total numbers for some of the cross tabulations.
Distribution of incident angina by employment grade and effort-reward imbalance tertiles at phases 1 and 5 of the Whitehall II study
Men and women from lower employment grades were more likely to have incident angina (table 1). Among men, a higher degree of effort-reward imbalance at phases 1 and 5 was associated with a higher risk of incident angina. However, among women, this association was only evident at phase 1. At phase 5, there does not appear to be much association between effort-reward imbalance and incident angina among women. A decrease in effort-reward imbalance was associated with lower risks of angina among men, but not among women. Relatively more men and women from lower grades experienced an increase in effort-reward imbalance.
Figure 2 shows the mean effort-reward imbalance ratio at phases 1 and 5 and the difference score between the two measures (phase 1 score minus phase 5 score) by employment grade, separately for men and women. There is a clear social gradient in effort-reward imbalance at phase 1 for both men and women, showing that those in higher employment grades have higher imbalance. However, at phase 5, this association is not so strong and the linear trend in effort-reward imbalance scores at phase 5 by employment grade is not as evident as for the phase 1 scores. When we look at the difference score, we see some evidence of a linear trend by employment grade. This suggests that those in the higher employment grades had reduced their imbalance (by phase 5) to a greater extent than those in the lower employment grades. The difference between the imbalance scores was greater for those in the higher grades. These mean trends were similar for men and women. As effort-reward imbalance has decreased, on average, from phase 1 to 5, hypothesis 3 can be restated as “does a reduction in effort-reward imbalance, over time, reduce the risk of angina?”.

Mean effort-reward imbalance (ERI) at phases 1 and 5 and the difference score by employment grade; Whitehall II study, men and women separately.
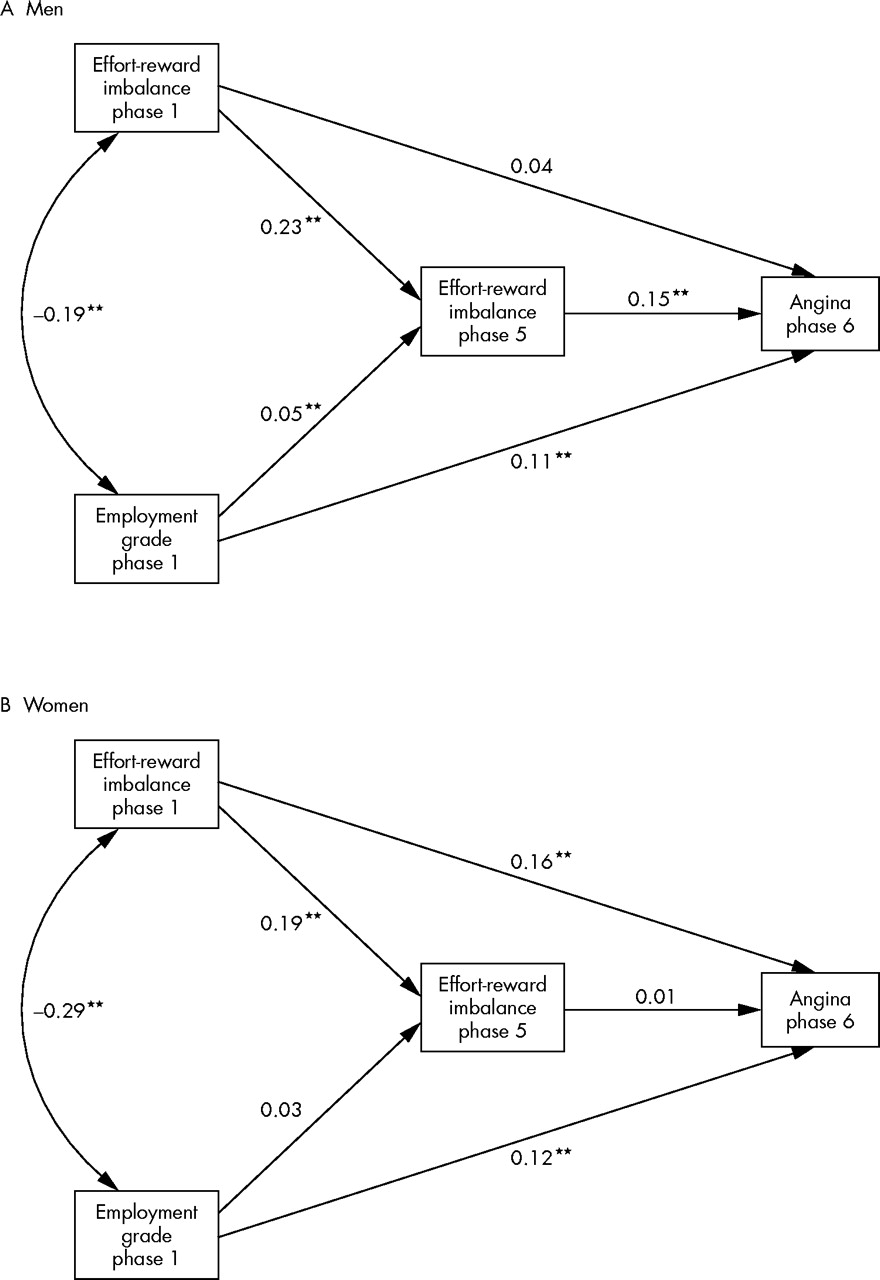
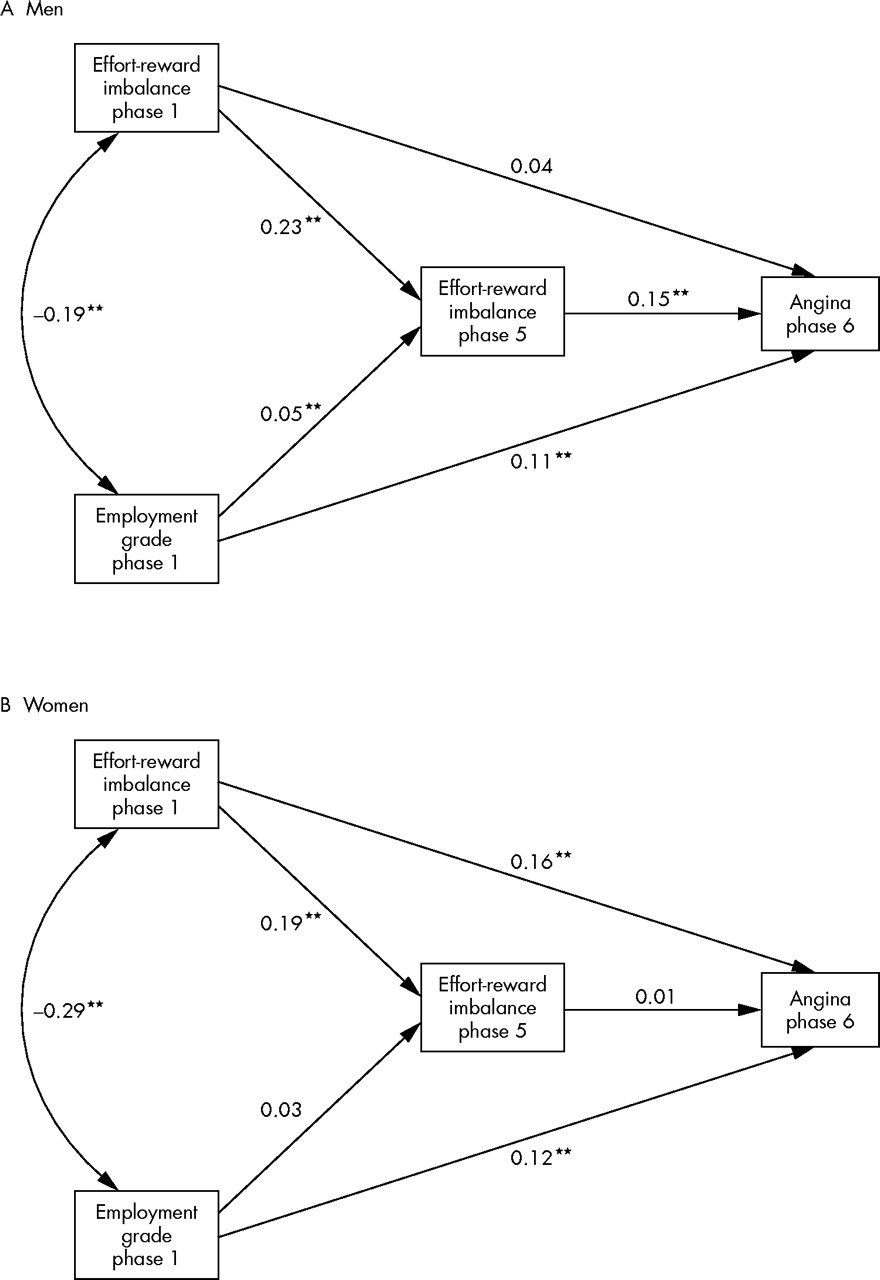
Figure 3 shows the results of the empirical test of the pathway model displayed in fig 1. All path coefficients in the figure are standardised probit coefficients. Among men, higher effort-reward imbalance at phase 5 is associated with incident angina. There is little evidence of a direct effect of imbalance at phase 1 on incident angina, although the indirect effect through imbalance at phase 5 was statistically significant (standardised probit coefficient of 0.17 with 95% confidence intervals from 0.08 to 0.25). This suggests that there is little evidence for hypothesis 2 (that effort-reward imbalance affects angina, adjusted for employment grade). However, when effort-reward imbalance at phase 5 is taken out of the model (that is, the path from imbalance at phase 5 to angina is set at zero), imbalance at phase 1 significantly affects incident angina, thus providing some evidence for hypothesis 2.
{kind=link}
{kind=link}
{kind=link}
Standardised probit regression coefficients for the model in fig 1; Whitehall II study. **p < 0.01.
Employment grade had direct and indirect effects (through imbalance at phase 5) on incident angina. Although the standardised indirect effect of employment grade on incident angina was small (0.01, with confidence intervals from 0.00 to 0.01), it was statistically significant at the 95% level. In other words, the effect of grade on angina is mediated, in part, by the effect of grade on effort-reward imbalance at phase 5. The negative correlation between employment grade and imbalance at phase 1 suggests that those in lower grades had lower effort-reward imbalance scores at phase 1, while the positive effect of grade on imbalance at phase 5 suggests that lower grades had higher imbalance scores at phase 5. Effort-reward imbalance at phase 1 was moderately correlated with imbalance at phase 5.
Among women, effort-reward imbalance at phase 5 appears to have little effect on angina. Imbalance at phase 1 and employment grade directly affect angina; there was little evidence of indirect effects through imbalance at phase 5. In summary, among women, empirical support is restricted to hypotheses 1 and 2 but there is little evidence to support hypotheses 3 and 4. Systolic blood pressure and body mass index were positively associated with incident angina (not shown in fig 3), although the only statistically significant association was between blood pressure and angina for men.
The probit coefficients in fig 3 for incident angina were converted into probabilities of incident angina for a person aged 45 at phase 1, with a BMI of 25 and systolic blood pressure of 120 mm Hg at phase 5 (table 2). These probabilities are calculated for a series of hypothetical people who had different combinations of these hypothesised minimum and maximum scores of effort-reward imbalance at phases 1 and 5. Not all such combinations are represented in the empirical data matrix of this study sample. Men and women who had consistently high effort-reward imbalance at phases 1 and 5 had the highest probability of incident angina. This was especially true for those in the lowest grades. Men who reduced their effort-reward imbalance (that is, those who had high imbalance at phase 1 and low imbalance at phase 5) had a lower probability of angina than those who had consistently high imbalance. Similarly, men who increased their effort-reward imbalance had a higher probability of angina compared to those who had consistently low imbalance or those who had decreased their imbalance (supporting hypothesis 3). Among women, those who reduced their effort-reward imbalance had similar probabilities of angina as those who had consistently high imbalance. Women who increased their imbalance from phase 1 to phase 5 has similar probabilities as those who had consistently low imbalance (not supporting hypothesis 3). This suggests that effort-reward imbalance at phase 5 does not affect incident angina and that effort-reward imbalance at phase 1 has a more important effect on incident angina among women from lower employment grades than imbalance at phase 5.
Probability of incident angina for a Whitehall II respondent (phase 5 to phase 6) aged 45 (at phase 1), with a BMI of 25 and systolic blood pressure of 120 mm Hg (at phase 5)
DISCUSSION
To our knowledge, this is the first report of adverse health effects produced by increases in adverse psychosocial work environments over time in terms of effort-reward imbalance. Among men, those who had increased their effort-reward imbalance had higher probabilities of incident angina than those whose imbalance had remained low or had reduced. This effect (of an increase in imbalance affecting angina) was not really evident for women. Due to methodological reasons results are restricted to the extrinsic component of this work stress model and, thus, may result in a potential underestimation of observed effects.
Further indirect support of the finding of an association between increase in stressful work over time and CHD risk in men comes from epidemiological studies that test the demand-control model in a longitudinal perspective. Theorell and Hallqvist22 reported an increased CHD risk among men who experience a decrease in their decision latitude at work. Another prospective study found increased mortality among those who were working in low-control jobs throughout their working life.23 Taken together, this information illustrates the usefulness of multiple assessments of an adverse psychosocial work environment. Presumably, data reflecting an exposure over the working life provide more explanatory power than a single measurement. Preliminary evidence of this conclusion was recently obtained from a study that showed the largest increase in risk of depression and psychosomatic symptoms among employees who exhibited continuously high level of effort-reward imbalance over time.24
Furthermore, among men, the social gradient in angina appears to be explained, in part, by the social gradient in the change in effort-reward imbalance. Although men and women in higher grades had higher imbalance to start with, they were more likely to reduce their imbalance later on. This resulted in a social gradient in the change in effort-reward imbalance (subtracting their later imbalance scores from their scores at the first time point). For men, those who had reduced their imbalance had lower probabilities of incident angina than those who had increased their imbalance (for women, this was not the case). As higher grade men were more likely to reduce their imbalance, the effect of employment grade on angina appears to be mediated, in part, by its effect on changes in effort-reward imbalance.
The fact that reductions in effort-reward imbalance contribute to the explanation of the social gradient in angina needs further consideration. As was shown, reductions were more frequent among civil servants from higher occupational grades. However, at phase 1, effort-reward imbalance was more pronounced among higher grades in this cohort who, subsequently, experienced the relatively largest reductions in stressful experience at work. How can this observation be explained? While several studies show higher mean scores of the effort scale in higher status groups, a reverse trend is usually observed with respect to the scores of the reward scales.12 In this study, comparable items measuring reward within the two questionnaires heavily focused on aspects of occupational career, in particular promotion prospects. It is possible that those in higher social positions obtain greater rewards from their work at a later stage in their career and that years of heavy investments are required in order to get promoted appropriately. Some of this “delayed gratification” may have been captured by differences in the two measurements of occupational rewards between phases 1 and 5. In contrast, lower grade civil servants experience very few promotion prospects as most of them are locked in a social position without upward mobility. It is therefore likely that a sense of relative deprivation with regard to occupational rewards grows over time that is reflected in a mean increase in the effort-reward difference score between phases 1 and 5.
Among women, there is evidence of a social gradient of angina. There is also some evidence of a direct effect of effort-reward imbalance at phase 1 on angina, although little effect of changes in imbalance on angina. However, the effect of employment grade on angina does not appear to be mediated through effort-reward imbalance at either time point. Although there is some evidence indicating that an adverse psychosocial environment outside work is likely to be more important in explaining CHD among women,25 any conclusion about the effect on effort-reward imbalance on CHD from this study may be premature due to the small number of incident angina cases among women, as well as gender differences in the self-report of angina (women are less likely to present angina symptoms to their doctor).
The association of effort-reward imbalance, assessed at study entry, with incident angina in men, is in agreement with previous findings from prospective studies. Results on this association among women are less consistent. Whereas several studies documented similar effects in men and women,8,9,14 other investigations, in addition to this study, failed to find an association of an adverse psychosocial work environment with CHD in women.26,27 This inconsistency could possibly be explained in terms of gender roles.28 Threats to work related social status are most stressful to the traditional male gender role as they endanger its core social identity, whereas women, in general, have alternative options of securing their social identity.29 Moreover, as pointed out earlier, an adverse psychosocial environment outside work, the home, may elicit more stressful reactions in women than the work environment. The elucidation of gender role related susceptibility to CHD following exposure to adverse psychosocial environments clearly requires further investigation.
The specific strengths of this investigation are the consistency of the reported findings with available evidence, the prospective study design, and the inclusion of information on change in adverse psychosocial work environments in terms of a theoretical model. There are also several study weaknesses and limitations to be discussed. First, angina and adverse psychosocial work conditions were measured by self-reported information. Reporting bias due to specific psychological traits or states (for example, negative affectivity), cannot be excluded.30 Yet, two arguments contradict this assumption. First, in previous analyses of the Whitehall II cohort, as well as in other studies, negative affectivity was measured and introduced as confounder into multivariate risk estimation, resulting only in a minor, non-significant reduction of the effect size on health produced by effort-reward imbalance.14,31–33 Second, a further prospective analysis of the association between effort-reward imbalance and risk of CHD in this cohort, based on clinical data (acute myocardial infarction, fatal and non-fatal CHD) over an 11 year follow up period, found significantly increased hazard ratios of CHD in civil servants with high scores in effort-reward imbalance.9 Additional evidence against the assumption of a spurious association due to bias comes from laboratory research and from investigations in natural settings (workplace) using ambulatory monitoring techniques. For instance, employees with a high effort-reward imbalance were shown to exhibit increased systolic blood pressure levels, increased heart rate, and reduced heart rate variability over the working day, compared to those without stressful experiences at work.34
A further limitation of the present study concerns the measurement of an adverse psychosocial work environment. As explained, the two measurements of effort-reward imbalance were not identical, and the intrinsic component of the model, over-commitment, was not included. Given the independent contribution of this latter variable to the estimation of CHD risk,9,29,35 we cannot rule out that reported effects are underestimated. Thus, a replication of findings based on identical measures and on the complete questionnaire defines a task for future research.
It has also been argued that a more comprehensive measurement of adverse psychosocial work conditions should be done by combining the effort-reward imbalance model with the demand-control model.21 In fact, this combined analysis has been executed in several prospective and case-control studies, indicating: (1) that the two models indeed measure different aspects of an adverse psychosocial work environment; (2) that each model contributes separately to the estimation of CHD risk; and (3) that the effect size of this estimation is about the same in either model.8,9,14,29,36
The reduced sample size resulting from restricted data available at phases 5 and 6 is a further issue of potential concern. Respondents from lower employment grades were more likely to have dropped out by phase 6, resulting in a possible under-estimation of the social gradient in CHD. Older respondents in employment were less likely to fill in the effort-reward imbalance questionnaire at phase 5, compared to younger respondents in employment. This may have resulted in an under-estimation of the effect of age on the outcome variables in the analyses. The statistical program used in the analysis, MPlus provides maximum likelihood estimation under missing completely at random and missing at random assumptions. This helps deal with the problem of drop out from the cohort by including predictors of drop out such as age and employment grade in the analysis.
An often stated additional criticism concerns the limited number of confounders included in psychosocial research on somatic diseases, such as CHD. It is argued that residual confounding may underlay the reported associations of psychosocial variables with somatic disease, thus precluding any firm evidence.37 It is hard to see how this critique can be maintained given the substantial replication of findings of an independent and significant contribution of distinct psychosocial variables to risk estimation of CHD (such as demand- control and effort-reward imbalance at work). These effects are sometimes attenuated by inclusion of multiple behavioural and biomedical risk factors, but it is rare that they are lost as a result of confounder control. In this paper, smoking, physical activity, body mass index, blood pressure, and diabetes were analysed as potential confounders (analysis not shown), but none of these risk factors was significantly associated with incident angina at phase 6. It is possible that increases in effort-reward imbalance at work result in increases in these cardiovascular risk factors (that is, they are mediators, rather than confounders), but such an analysis is not yet possible on the Whitehall II data.
Finally, the findings of this study are restricted to a specific occupational group, male and female civil servants in the United Kingdom. It is uncertain to what extent they can be generalised to other occupational groups and countries. However, as associations of effort-reward imbalance at work with CHD have been observed in other occupational groups, such as blue-collar workers in Finland8,38 and in Germany,35 it is unlikely that civil servants define a special case in this regard.
As robust evidence on health adverse effects of effort-reward imbalance is available,8,9,12–15,31–33,35 specific intervention measures can be derived from this model at the structural, interpersonal, and personal level. Structural measures include the strengthening of monetary and non-monetary gratifications and the improvement of promotional opportunities. At the interpersonal and personal level, enhanced leadership skills, appropriate feedback to co-workers, and balanced ways of coping with workload are targets of intervention. First results of intervention studies along these lines are promising.39
In conclusion, despite the limitations mentioned, this investigation found consistent associations of effort-reward imbalance at work at study entry, and of changes in imbalance over time, with risk of incident angina in male civil servants. Furthermore, the social gradient in angina among men is explained, in part, by change in level of work stress over time according to occupational class. These findings contribute to a considerable amount of evidence on the detrimental health effects produced by an adverse psychosocial work environment. Given this evidence, the design and implementation of theory based intervention measures seems to be a timely challenge.
Acknowledgments
The Whitehall II study has been supported by grants from the Medical Research Council; British Heart Foundation; Health and Safety Executive; Department of Health; National Heart Lung and Blood Institute (HL36310), US, NIH: National Institute on Aging (AG13196), US, NIH; Agency for Health Care Policy Research (HS06516); and the John D and Catherine T MacArthur Foundation Research Networks on Successful Midlife Development and Socio-economic Status and Health.
The authors thank all participating civil service departments and their welfare, personnel, and establishment officers; the Occupational Health and Safety Agency; the Council of Civil Service Unions; all participating civil servants in the Whitehall II study; and all members of the Whitehall II study team. The authors also thank Annie Britton for helpful comments on an earlier draft of this paper.
REFERENCES
Footnotes
-
Competing interests: none declared
-
Ethical clearance: Ethical approval for the Whitehall II study was obtained from the University College London Medical School Committee on the ethics of human research. The Whitehall II study participants gave written, informed consent, and the manuscript conforms to the principles outlined in the Declaration of Helsinki.