Article Text

Abstract
Background Studies have shown that serum low-density lipoprotein (LDL-C) and non-high-density lipoprotein (non-HDL-C) have recently declined in the USA among adult and child populations despite high obesity prevalence rates. The purpose of this study was to assess whether there was a significant linear decrease in LDL-C and non-HDL-C, but not Body Mass Index (BMI) percentile among a cross-sectional, large, homogenous cohort with consistent methodology over the past decade.
Methods A total of 47 198 children, mostly between 10 and 11 years old, participating between 2002 and 2012 were examined to assess trends in serum lipid concentration and BMI percentile.
Results For LDL-C, year of screening was significant (p<0.0001) even with the inclusion of gender, age and BMI (all p<0.0001). For non-HDL-C, year of screening was also significant (p<0.0001), even with the inclusion of gender (p=0.0445), age (p<0.0001), BMI (p<0.0001) and systolic blood pressure (p=0.0021). Although some non-linear trends were also significant (eg, a quartic trend, p<0.001), the linear trend provided the best fit for both cholesterol models. By comparison, we noted general maintenance of BMI percentile over time.
Conclusions Between 2002 and 2012, among 5th grade Appalachian children, there was a consistent linear decrease in LDL-C and non-HDL-C despite continued high prevalence rates of obesity, diabetes and hypertension. The improvement in LDL-C and non-HDL-C could be due to multifactorial causes.
Statistics from Altmetric.com
The USA and other nations have noted persistent increases or maintenance of prevalence of age-adjusted and gender-adjusted Type II diabetes mellitus and obesity.1 ,2 Despite these increases in related cardiovascular risk factors, the past few decades have seen the emergence of decreases in age-adjusted trends in blood cholesterol levels. Previously, studies such as the Framingham Offspring Study3 and Bogalusa Heart Study4 noted secular trends increasing in young adults and adolescent children in the late 1980s and early 1990s. The first studies to note maintenance and/or decreases in low-density lipoprotein cholesterol (LDL-C) after controlling for age and obesity in the USA in adults in the early 1990s included the Minnesota Heart Survey5 and other studies from European countries.6 ,7 This decreasing secular trend was subsequently noted among young adults in the Coronary Artery Risk Development in Young Adults Study in 1996,8 and among young adults in Europe with the Cardiovascular Risk in Young Finns Study.9
The National Health and Nutrition Examinations Surveys (NHANES) have been used to examine the trends in cholesterol levels across the US population in adults and children. Three cohorts of NHANES (1976–1980; 1988–1994; 1999–2006) experienced decreases in total cholesterol (TC), LDL-C and non high-density lipoprotein (non-HDL-C) among adults, although similar trends were not seen for triglycerides (TRIG) or obesity rates.10 ,11 Cohen and colleagues10 note that self-reported high cholesterol substantially increased over time, and thus, suggesting increased awareness and treatment of high cholesterol likely contributed to that decrease. Similarly, the 1988–1994, 1999–2002 and 2007–2010 youth cohorts were also examined and found to have generally decreasing LDL-C over time. However, a slight increase was noted in the younger groups in mean lipid levels from the 1998–1994 to the 1999–2002 cohorts.12
These mean lipid decreases are generally thought attributable (although not proven) to be due to a range of population-based initiatives, including increased use of lipid-lowering pharmacological treatment, promotion of healthy diet including low saturated fat intake, appropriate physical activity and abstinence from tobacco use.10 ,12 ,13 This is consistent with recent findings demonstrating high-income regions (eg, Australasia, North America and western Europe) showing mean TC declines14; findings which lend themselves to recommendations that similar nutritional policies and pharmacological interventions be used to accelerate improvements in TC in low-income and middle-income regions. Not everyone is so optimistic: de Ferranti noted that other explanations are worth exploring, including inaccuracies due to changes in methodology (eg, for NHANES) and the possibility that the positive changes are only temporary.13 de Ferranti noted the positive changes in cholesterol unlikely to be due (for US youth) to increases in prescription drugs or healthier lifestyles particularly given the obesity increases; rather, the trend is likely due to decreases in transfats on the population level.13
West Virginia (WV), a rural, medically underserved Appalachian state, has some of the highest prevalence rates of adult obesity, diabetes and high blood pressure in the nation.15 Concerned with these alarming statistics, the state passed legislation in 2005 (WV HB 2816) entitled the West Virginia Health Lifestyles Act that consisted of five school-based mandates that required health education assessments, fitness assessments, modest increases in physical education, Body Mass Index (BMI) assessments and the availability of healthy beverages in schools.
In summary, research generally (but not consistently) demonstrates decreases in LDL-C and non-HDL-C in adults and children since the 1980s. The goal of this study was to examine a large cross-sectional WV dataset for youth (5th grade, generally 10–11 years of age) over the past decade to determine if there were linear decreases over that time period in LDL-C and non-HDL-C levels (consistent with previous research). This dataset lends itself to uniquely examine the research question with a large span of data points over time in a region of the USA with poor cardiovascular outcomes, but where the region has taken steps to improve these health outcomes. We hypothesise that there will be a consistent linear decrease in LDL-C and non-HDL-C over the decade despite continued high prevalence of obesity, diabetes and high blood pressure.
Materials and methods
The Coronary Artery Risk Detection In Appalachian Communities (CARDIAC) Project started as a small school-based cardiovascular disease (CVD) surveillance project piloted in three rural WV counties in 1998. It has grown to an expanded multidimensional screening, research and intervention effort involving all 55 WV counties and over 480 schools. To date, more than 165 000 children from select grades have received free health screening through the programme. This is particularly important given the limited per capita income of families living in the state and the need to provide health screenings to all children.16 For over a decade, CARDIAC has provided information to participating families, communities, the state and nation17 about chronic illnesses including hypertension, abnormal blood lipids and obesity18 ,19; asthma20; prediabetic conditions21; health behaviours22; and intervention factors.23 Average findings for the programme period demonstrate that from 1998 to 2013, 47.1% of fifth grade students in WV were either overweight (BMI percentile 85–94.9th) or obese (BMI percentile >95th). More information about CARDIAC can be found on the website at http://www.cardiacwv.org. Only fifth grade participants receive fasting lipid profiles (FLP), and thus, are the only participants included in this study.
West Virginia University Institutional Review Board approved the study protocol for the Protection of Human Subjects, and written consent forms were sent to parents. Individualised health screening reports from the project were sent home to all participating children and their parents. Aggregate data is available by county and year through http://www.cardiacwv.org. With this active consent process, response rates for fifth grade participants by year ranged from 31% to 49% since 1998. Our previous work has shown that the differences between participants and non-participants are minimal. Non-participants are less likely to have a primary care provider and to have health insurance, but there is no difference in BMI or any other demographic variables analysed in the present study.24
Measures
The comprehensive risk screening for fifth grade participants included calculation of BMI from height and weight, resting diastolic blood pressure and systolic blood pressure (SBP), and a FLP, which included measured TC, HDL-C, LDL-C, and TRIG. Non-HDL-C was calculated by subtracting HDL-C from TC. Children were asked to fast for 12 h prior to the screening.
Children's height (cm) and weight (kg) were measured using the SECA Road Rod stadiometer (78″/200 cm) and the SECA 840 Personal Digital Scale. Students were asked to remove shoes prior to height and weight measurements. These measurement were used to determine the child's BMI and BMI percentile, calculated using CDC Epi Info V.3.5.4 software.25
Blood pressure was taken after the child has been resting for 5 min. The first Korotkoff sound was used to record systolic pressure and the fifth Korotkoff sound was used to record diastolic pressure.
All cholesterol levels were obtained in either a private area of the school or children were given a voucher to have a FLP conducted in a local laboratory (LabCorp) or hospital. Prior to 2002, cholesterol was taken using a finger-stick method. If the values were high, vouchers were given to the student to have a FLP done at a local lab. Starting in 2002, vouchers and/or FLP were conducted. Thus, data analysed in this manuscript start in 2002, and do not include any finger-stick-obtained cholesterol levels (1998–2002), in order to avoid potential bias due to different methods of cholesterol measurements. Consistent blood specimens were taken since 2002, and all labs (ie, hospital or LabCorp) used consistent methods to process the specimens.
Statistical analysis
Data for CARDIAC were stored in IBM SPSS Statistics V.2126 software. All analyses conducted in this manuscript used SAS V.9.327 software. Only participants with completed FLP data were included in these analyses; in the event of missing data on other variables, missing data were treated with pairwise deletion. Orthogonal contrast matrices were used to test the hypothesis of a linear (vs a non-linear) trend over time for LDL-C and non-HDL-C values. Contrasts were assigned for each year from 2002 to 2012, for a total of nine different levels of orthogonal polynomial contrast matrices using the ORPOL function in PROC IML, generally considered a traditional approach to examining linear versus non-linear trends.28 A generalised estimating equation (GEE) model was constructed to predict variance in LDL-C, non-HDL-C and BMI percentile between 2002 and 2012, with school identification number nested within year of screening for the repeated measures term. GEE is an extension of generalised linear models (GLM) that provides a semiparametric approach to longitudinal data analysis. It is a marginal model, used to describe the mean response (ie, the marginalised mean) over individuals at each time point specified in terms of fixed-effect covariates. Within-person correlation and association over time is incorporated into the estimation methodology. All available demographic, family history and variables typically associated with higher cholesterol levels (such as BMI and SBP) were included as covariates; prior to inclusion, covariates had to have significant bivariate relationships with LDL-C and non-HDL-C. Only demographic variables were included in the BMI percentile model.
Results
Between 10 and 11 years of age, 5th grade children numbering 471 98 participated in a cross-sectional statewide CARDIAC screening between 2002 and 2012, and had a complete FLP. Consistent with state demographics, 92.6% were Caucasian and 53.6% female. LDL-C (M=92.9, SD=25.5) and non-HDL-C (M=111.0, SD=28.9) cholesterol levels were normally distributed. Covariates included race, gender, age in years (M=10.5, SD=0.6), SBP (M=108.6, SD=11.75) and BMI (M=21.36, SD=5.2).
Models predicting LDL-C and non-HDL-C were significant and fit a linear trend (p<0.0001) attributable to the explanatory variables. Although some non-linear trends were also significant (eg, a quartic trend, p<0.001), the linear trend provided the best fit for non-HDL-C (figure 1) and LDL-C (figure 2) models.
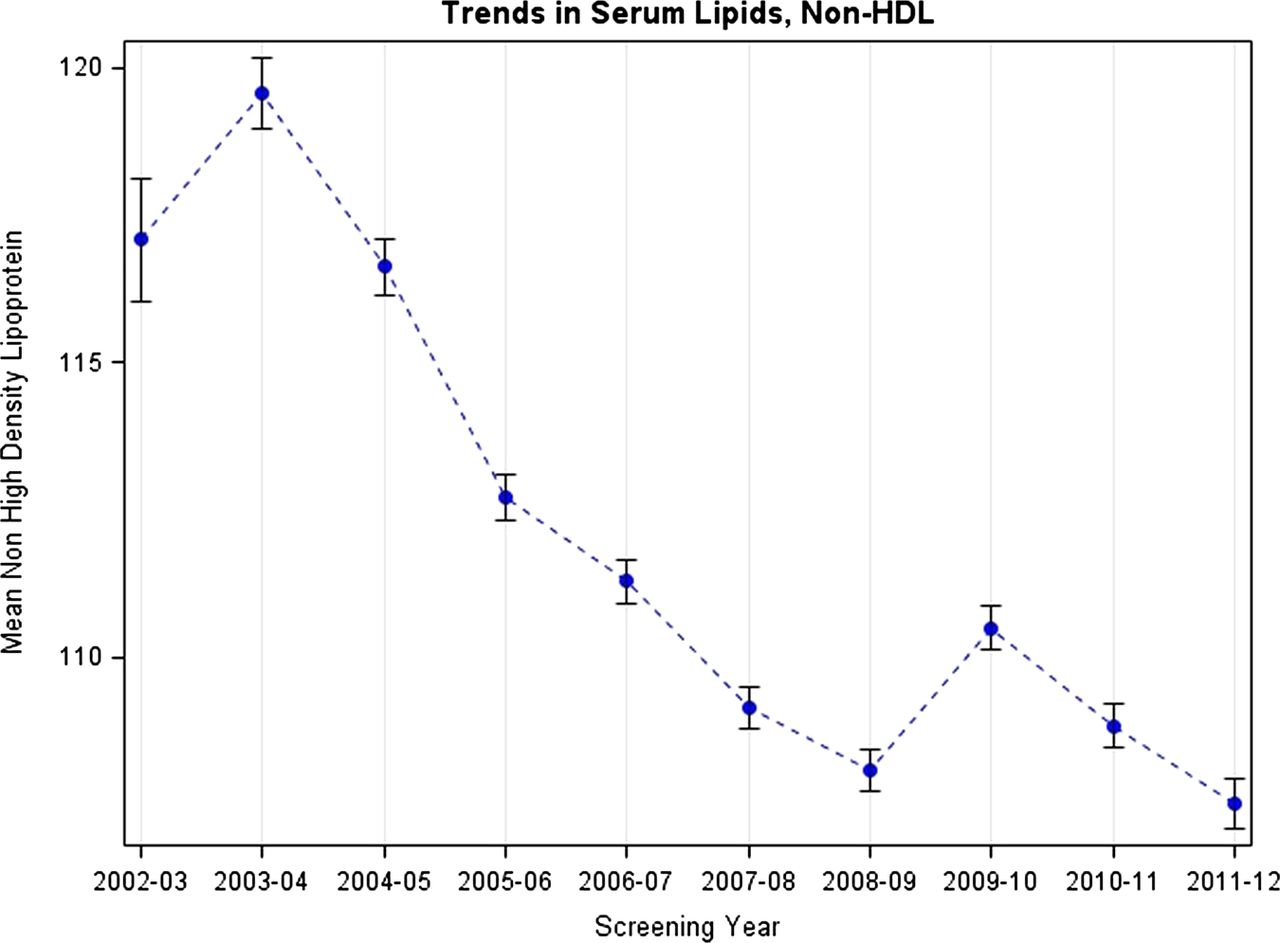
Bar graph of average non-HDL-C in mg/dL, with SEs, from 2002–2012 (n=45 077).
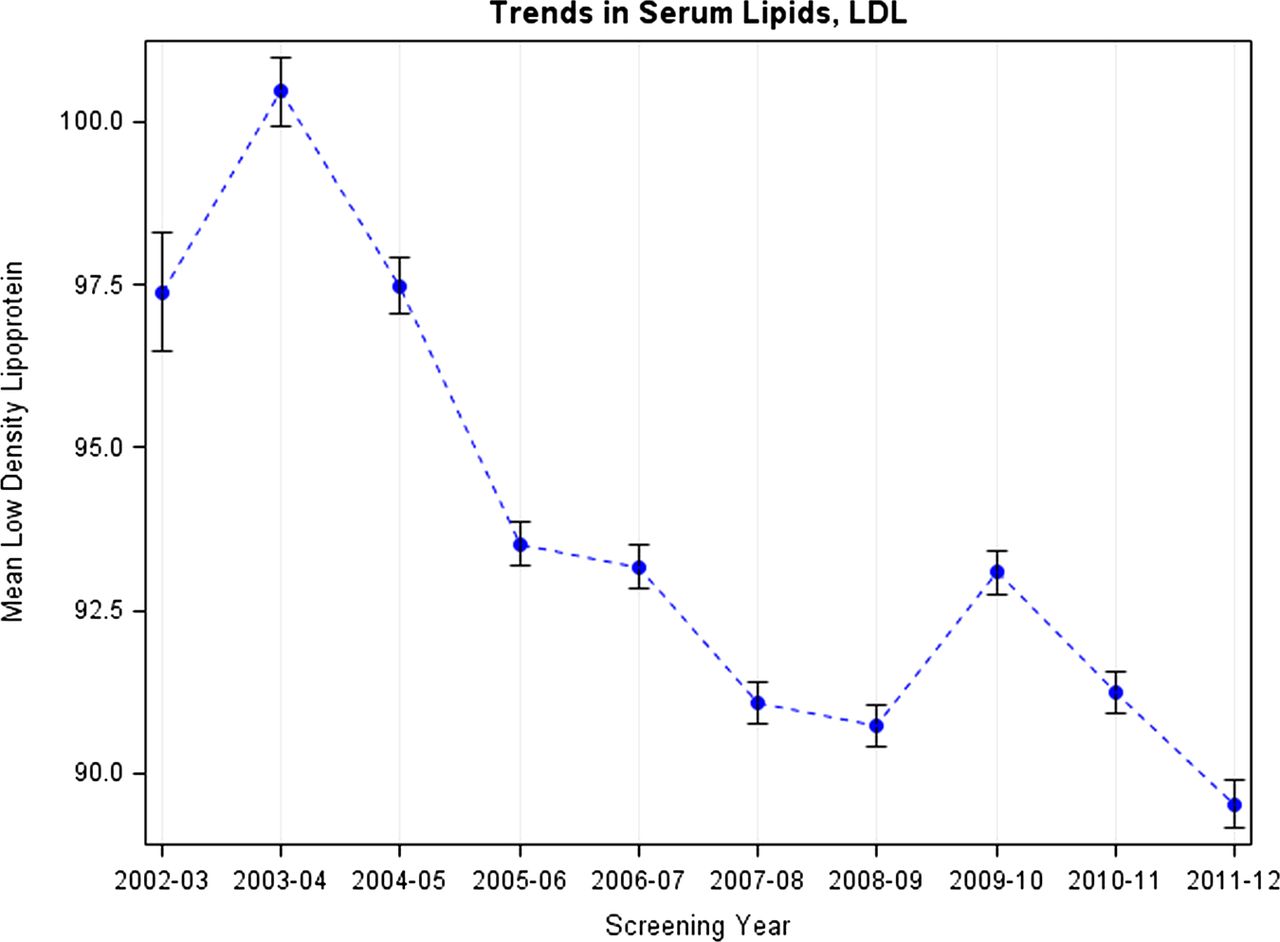
Bar graph of average LDL-C in mg/dL, with SEs, from 2002–2012 (n=46 779).
For non-HDL-C (table 1), year of screening was significant (p<0.0001), as was gender (p=0.0445), age (p<0.0001), BMI (p<0.0001), and SBP (p=0.0021). For LDL-C (table 2), year of screening was significant (p<0.0001) as were gender, age and BMI (all p<0.0001).
GEE regression predicting variance in non-HDL-C (n=45 077)
GEE regression predicting variance in LDL-C (n=46 779)
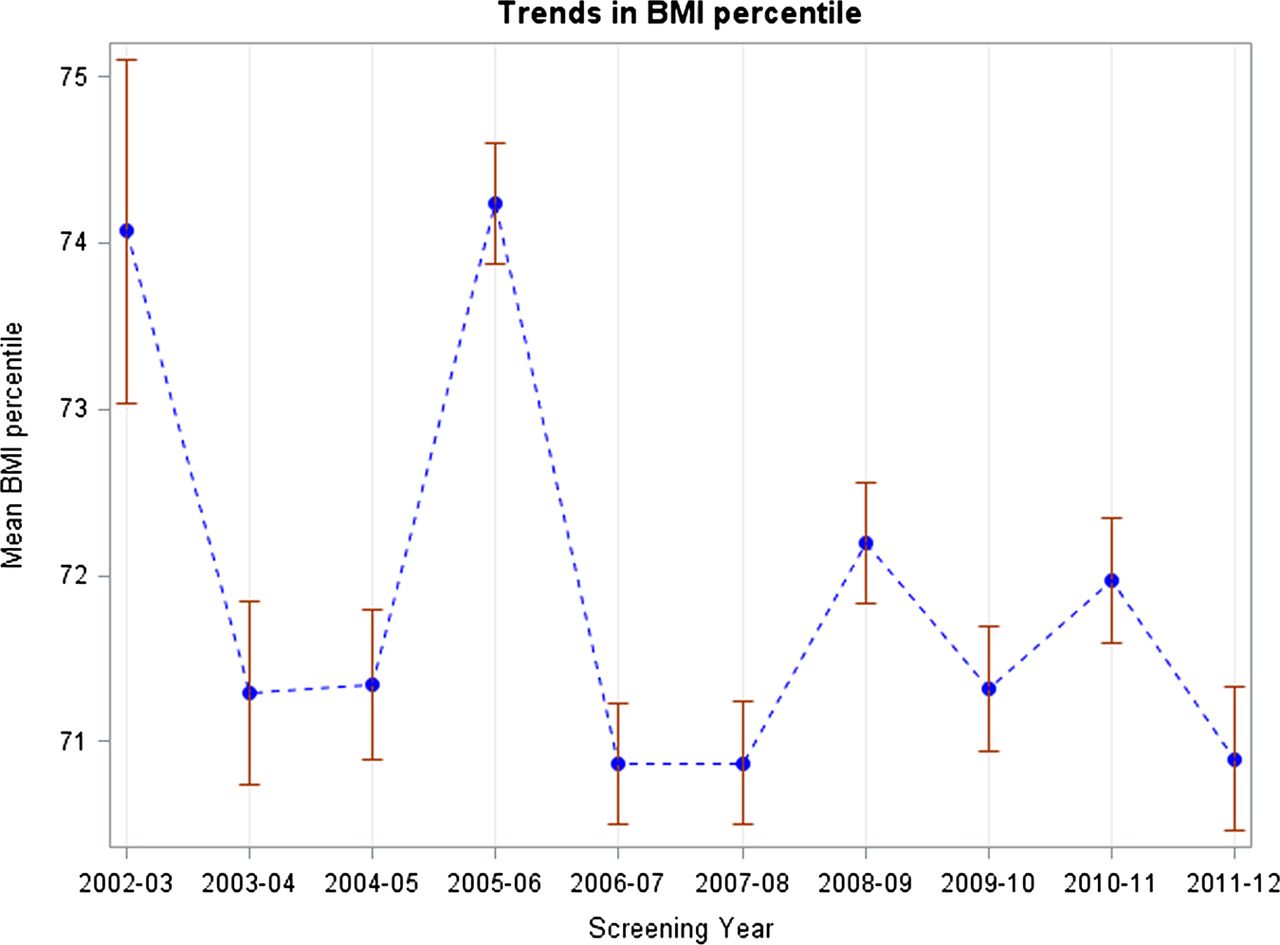
For comparison purposes, we also analysed BMI percentile for the yearly trend (figure 3). Specifically, year of screening was significant (p<0.0001), as were covariates of gender (p<0.001), age (p=0.032) and race (p<0.0001). However, when compared with the final year of data collection (2011–2012), year of screening was only significant for 2002–2003 (estimate=3.02, SE=1.49, p=0.043) and 2005–2006 (estimate=3.35, SE=1.02, p<0.0001). The linear trend was not significant for BMI percentile across years (p=0.057), whereas other trends including the quintic (p=0.004) and octupic (p<0.0001) trends fit the data, suggesting a general maintenance of children's BMI percentile in the WV Appalachian region between 2002 and 2012.

{kind=link}
{kind=link}
{kind=link}
Bar graph of average Body Mass Index percentile with SEs, from 2002–2012 (n=47 198).
Discussion
There was a decreasing linear trend in LDL-C and non-HDL-C (but not in BMI percentile) over the past decade among 5th grade Appalachian children. This finding is consistent with previous literature among adults10 and children.12 This study has the additional benefit of consisting of a large span of data points over time in a region of the USA with poor cardiovascular outcomes, but where the region has taken steps to improve these health outcomes. Additionally, this study makes use of advanced GEE repeated-measures modelling and examines other types of trends (besides a simple linear model) to determine the presence of linear trends over time.
Although not a focal point of this manuscript, there may be some interest in additionally interpreting the covariates included in the model. First, race and SBP were only significant for the bivariate correlation with non-HDL-C (not LDL-C); the predictor within the non-HDL-C regression demonstrated that in this generally homogenous, Caucasian, Appalachian sample having a lower SBP and being of African–American or biracial race may be protective against higher non-HDL-C (but not LDL-C). This may be an artefact of the limited minority racial make-up of the sample. Additionally, gender had a variable effect depending on type of cholesterol (female was protective for LDL-C but not non-HDL-C), which may be due to lower cholesterol levels during puberty occurring at younger ages among females. Being older in age (again, possibly a puberty-driven artefact of the data) and having a lower BMI were also protective factors in these analyses.
This study has several limitations that should be considered. For example, this data is cross-sectional, and differences over time may be due to cohort trends rather than population reductions in cholesterol. Given the consistent findings with previous literature among children and adults, this explanation seems unlikely. However, the cross-sectional nature of the data should caution against any causal extrapolation. Additionally, these findings are limited to the generally rural, homogenous Appalachian population of WV, and may not be applicable to other areas. No indicator of socioeconomic status was consistently available across these study years. Future studies may wish to include an indicator such as family income. Despite these limitations, the strengths of the manuscript (the large sample over an extended period of time, nested within a large number of schools across a large Appalachian area, with homogeneous methodology) demonstrate consistent linear drops in cholesterol levels over a 10-year period among a medically underserved, high-risk population.
Several possible explanations for the decreases in LDL-C and non-HDL-C are worth considering. Similar to explanations found in the literature, it is possible that the improvements in serum lipids are the result of interventions for CVD, lifestyle modification, pharmacotherapy, or healthier lifestyles in general.10 ,12 ,13 In particular, WV has made strides in the past decade by passing legislation improving child nutrition in schools and reducing non-healthy beverage options in schools. WV also has active intervention initiatives to improve physical activity in the schools, such as increasing active video game use in schools, building walking paths and establishing a state physical activity plan. However, it must be noted that the obesity prevalence is high despite these intervention efforts, and it appears the cholesterol trend started decreasing prior to many of these efforts taking place. The same limitation must be placed on possible increases in soy proteins, which have favourable impact on lipids and weight.29 ,30 Similarly, we do not believe that these decreases are due to corresponding increases in pharmacotherapy, as the authors of this manuscript conduct preventative cardiology clinics throughout the state, and have not seen any children who were put on statins without consultation and referral. The authors also do not believe that there has been any significant change in the incidence of genetic dyslipidaemias among children in this cohort. A drop in prevalence of familial hyperlipidaemia or familial combined hyperlipidaemia (LDL-C levels ≥160) could potentially skew results, but given the relatively low incidence of these disorders each year, it is difficult to state with distinct certainty if there has been a significant decline, let alone a decline meaningful enough to contribute to the decreasing trends that have been observed.
Thus, we suggest that the improvement in LDL-C and non-HDL-C is due to the decline in intake of saturated and trans-fats at a population level in the past several decades. The suggestion of trans-fats as driving this trend has been proffered before13; however, late into the 1990s, trans-fats were commonly found in nearly all cookies and crackers, among other foods. Legislation for labelling trans-fats became effective in 2006. Again, the trends in decreasing LDL-C started prior to these initiatives. One possible explanation may be the Nutrition Labeling and Education Act (NLEA) implemented in 1994,31 combined with public health recommendations to reduce fat intake starting in the late 1970s.32 This assisted in a consumer-driven increase in ‘low-fat’ food, generally decreasing saturated fats, which is also linked to improving LDL-C levels.33 This may have initially improved LDL-C levels as the ‘low-fat’ food availability spiked in the 1990s. Unfortunately, saturated fats were replaced with vegetable fats or added sugars. One analysis of children's diets in the 1990s showed that although children's intake of fat as a percentage of calories decreased over the decade, their caloric intake actually increased, and a large portion of their food energy came from added sugars.34 Consistent with population-based study results in Poland,35 this restriction of saturated fats must be paired with low intake of trans-fatty acids for continued improved cardiovascular health. Governmental regulations have continued through the past decade to improve labelling and restriction of trans-fats, with corresponding decreases in trans-fats from 2007 to 2011.36
Conclusions
The mean values for LDL-C and non-HDL-C of a cross-sectional sample of children in 5th grade Appalachia have decreased over time even after adjusting for age, BMI, gender, race and SBP. Consistent with the literature, this favourable trend in decreasing LDL-C levels was not accompanied by comparable decreases in obesity rates. The initial decrease in saturated fats followed more recently by a decrease in trans-fats from many foods over the past two decades is a likely and more plausible contributor to this downward trend in the serum lipids.
What is already known on this subject?
-
Serum low-density lipoprotein (LDL-C) and non high-density lipoprotein (non-HDL-C) have recently declined in the United States among adult and child populations despite high obesity prevalence rates.
What this study adds?
-
Study results show a significant linear decrease in LDL-C and non-HDL-C among a large, homogenous cohort with consistent methodology over the past decade. This favourable trend in decreasing serum lipid levels was not accompanied by comparable decreases in BMI percentile. The initial decrease in saturated fats followed more recently by a decrease in trans-fats from many foods over the past two decades is a plausible contributor to this downward trend in the serum lipid levels.
References
Footnotes
-
Contributors All authors contributed equally to the work. CLL, conceptualised and designed the study, drafted the initial manuscript, and approved the final manuscript as submitted. YDG, carried out the initial analyses, reviewed and revised the manuscript, and approved the final manuscript as submitted. LC, is the Vice Chair of Research for the Department of Pediatrics, critically reviewed the manuscript, and approved the final manuscript as submitted. CJ, works with CARDIAC participants attending the Familial Hypercholesterolemia Clinic and at Preventative Cardiology Clinics, critically reviewed the manuscript, and approved the final manuscript as submitted. WN, is the director of the CARDIAC project, critically reviewed the manuscript, and approved the final manuscript as submitted.
-
Funding This work was supported by the WV Bureau for Public Health and the Claude Worthington Benedum Foundation.
-
Competing interests None.
-
Ethics approval Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.