Article Text

Abstract
Background: Socioeconomic gradients in the occurrence of myocardial infarction are well known, but few studies have examined socioeconomic disparities in post-infarction outcomes. The objective of this study was to explore relations of socioeconomic status with the incidence, treatment, and outcome of first coronary event in Rome, Italy, during the period 1998–2000, examining effect modification by gender.
Methods: Subjects were Rome residents aged 35–84 years who died from first acute coronary event before reaching the hospital (n = 3470) or were hospitalised for first acute myocardial infarction (n = 8467). Area based deprivation status and patients’ educational attainment were the exposure variables. The outcomes were: incidence of coronary event; recanalisation at the index hospitalisation and fatality within 28 days of hospitalisation; cardiac readmissions and fatality between 28 days and one year of index hospitalisation.
Results: Incidence rates increased as area based deprivation status increased; the effect was stronger among women than among men (men RR = 1.40, 95%CI:1.30, 1.50, women RR = 1.78, 95%CI:1.60, 1.98, most compared with least deprived). Rates of recanalisation were significantly lower in the most deprived patients than in the least deprived (OR = 0.77, 95%CI:0.59, 0.99) and in the less educated than in the highly educated (OR = 0.73, 95%CI:0.58, 0.90). Associations of short term fatality with area based deprivation status and educational attainment were weak and inconsistent. However, neither deprivation status nor education was associated with one year outcomes.
Conclusions: Area based deprivation status is strongly related to incidence of coronary events, and more so among women than among men. Deprivation status and educational attainment are weakly and inconsistently associated with short term fatality but seem not to influence one year prognosis of acute myocardial infarction. Deprived and less educated patients experience limited access to recanalisation procedures.
- SES, socioeconomic status
- AMI, acute myocardial infarction
- COPD, chronic obstructive pulmonary disease
- PTCA, percutaneous transluminal coronary angioplasty
- CI, confidence interval
- HR, hazard ratio
- RR, relative risk
- OR, odds ratio
- sudden cardiac death
- health services accessibility
- myocardial infarction
- social class
Statistics from Altmetric.com
- SES, socioeconomic status
- AMI, acute myocardial infarction
- COPD, chronic obstructive pulmonary disease
- PTCA, percutaneous transluminal coronary angioplasty
- CI, confidence interval
- HR, hazard ratio
- RR, relative risk
- OR, odds ratio
Coronary heart disease remains a leading cause of death in industrialised countries, but its incidence is not evenly distributed in the population. Socioeconomic gradients in the occurrence of myocardial infarction are well known,1–3 and are related to disparate lifestyle risk factors; however, inequitable access to primary care and discrepancies in treatment and adherence may also be involved. After an acute coronary event, the efficacy of health care during both the acute phase and later medical follow up influences probability of survival.4,5
The literature on post-hospitalisation outcomes of myocardial infarction contains conflicting results. North American studies found that after adjusting for baseline characteristics, low socioeconomic status (SES) was significantly associated with mortality.6–8 However, a recent Canadian study found no significant association between SES and mortality up to one year after hospitalisation.9 In Europe, fatality rates in the first month were significantly higher among less privileged patients in Finland3 and England,10 but not Scotland1; increased mortality in the first year was associated with low SES in Finland,3 but not England.10 Results on inequities in non-invasive treatments for cardiovascular disease are inconsistent.9–12 In many locations, underprivileged groups are less likely to receive invasive and diagnostic procedures and more likely to experience delays in these types of care.6–8,13,14
Our objective was to examine the relations that SES had with the incidence, treatment, and outcome of first coronary events in Rome, Italy, between 1998 and 2000. Because myocardial infarction rates are different in men and women,15 we also evaluated effect modification by gender.
METHODS
Data
This study is based on administrative data. The Regional Cause of Death Registry lists the causes of death, coded according to the International Classification of Diseases, 9th edition (ICD-9), for all residents of the Lazio region, where Rome is located. The regional hospital discharge registry covers 96% of public and private hospitals in Lazio. Specific training programmes for personnel (physicians and administrators) are periodically provided in each hospital to improve the quality of coding. The regional health authority routinely checks data quality from all hospitals in the region.16 Information about each hospital discharge includes patient characteristics, diagnoses, and surgical interventions (ICD-9). The municipal registry maintains records on all official residents of Rome, including vital status and dates of birth and death. Fiscal codes, used as identifiers in record linkages, are based on name and date and place of birth and are present (or calculable from data present) in all government records including the aforementioned registries.
Residents of Rome aged 35–84 who died from acute coronary events before reaching a hospital (out of hospital deaths) were selected as follows: deaths during 1998–2000 with causes ICD-9 = 410–414 were found in the regional cause of death registry and linked with the regional hospital discharge registry. We excluded subjects who died out of hospital within 28 days after hospitalisation for either acute myocardial infarction (AMI) (ICD-9: 410), to avoid duplicating hospitalised subjects, or ischaemic diseases (ICD-9: 411–414), to exclude people who probably did not suffer an AMI. All deaths occurring in a hospital or immediately preceded by a hospitalisation from causes other than ischaemic heart disease were excluded, as AMI was considered a complication.
Hospitalised AMI cases, retrieved from the regional hospital discharge registry, were all residents of Rome aged 35–84 years who were admitted to hospitals during the years 1998–2000 with principal diagnosis of AMI (ICD-9 = 410). Patients were excluded if they were discharged alive after fewer than three days, an indication that AMI was ruled out.
Our goal was to study “first” coronary events. We therefore excluded all hospitalisations that included a secondary diagnosis of previous infarction (ICD-9 = 412) and all subjects with a prior hospitalisation for AMI or previous infarction in the calendar year of the index event or in the three preceding years.
Follow up data on vital status and cardiac readmissions to the end of 2001 for hospitalised patients were obtained by linking the respective aforementioned registries.
For each person, comorbidities in the three years before the event were identified via record linkage. Hospitalisations with any of the following principal or secondary diagnoses were flagged: diabetes (ICD-9 = 250), hypertension (ICD-9 = 401–405), chronic obstructive pulmonary disease (COPD) (ICD-9 = 490–496), peripheral vascular disease (ICD-9 = 440.2), angina/other chronic ischaemic heart disease (ICD-9 = 413–414), conduction disorders (ICD-9 = 426), arrhythmia (ICD-9 = 427), or heart failure (ICD-9 = 428). At the index event for hospitalised patients, presence of these illnesses as secondary diagnoses was noted, as was recourse to recanalisation procedures (ICD-9 procedure = 36.0), hereafter abbreviated PTCA (percutaneous transluminal coronary angioplasty, ICD-9 procedure = 36.01, 36.02, 36.05, representing 95% of recanalisations performed on the cohort). Bypass surgery rates were too low to be examined.
Rome has a total population of 2 576 866 residents living in 5550 census blocks. The population aged 35–84 years, used as the denominator in this study, is 1 602 468. Each subject’s area based deprivation status was derived from an index based on multiple characteristics of the census block of residence from 1991 census data: distribution of educational level, occupational categories, working age male unemployment rate, family size, crowding, and proportion of dwellings rented/owned. The city distribution of this index was divided into four categories by the 20th, 50th, and 80th centiles; these categories (1 = least deprived, 4 = most deprived) comprised the deprivation status variable used in this study. Area based deprivation status is available for 97.3% of Rome’s total population.17
For hospitalised cases only, discharge records included patients’ individual levels of education, which were aggregated into three categories: fewer than eight years of education (no middle school diploma), 8–12 years (middle school diploma), and at least 13 years (high school diploma or more).
The administrative nature of the data rendered ethics committee approval unnecessary.
Data analysis
Incidence rates (out of hospital deaths, hospitalisations, total events) in the Rome population aged 35–84 years were calculated by area based deprivation status, stratified by gender, standardised for age (direct method, five-year age classes, world standard population), and reported as annual rates per 100 000 persons. Age adjusted relative risks (RR) and 95% confidence intervals (CI) were estimated using Poisson models.
Within the hospitalised cohort, separate associations of area based deprivation status and educational attainment level with several outcomes were examined. Patients whose deprivation status or educational attainment was missing were excluded from the respective analysis. Crude rates were calculated before modelling. Short term outcomes studied were receipt of PTCA at index hospitalisation and fatality within 28 days of hospital admission. Logistic regression analyses yielded adjusted odds ratios (OR) for deprivation status and educational attainment, respectively, using the most privileged category as the reference. Those surviving at least 28 days were followed up until 365 days after the index event; outcomes studied were fatality, hospital readmission for new AMI, and hospital readmission for other cardiac causes: angina/other acute ischaemic heart disease (ICD-9 = 411, 413), arrhythmia (ICD-9 = 427), or congestive heart failure (ICD-9 = 428). For these outcomes, Cox multivariate models yielded hazard ratios (HR) by deprivation status and educational attainment.
For all analyses, several baseline characteristics were considered a priori as potential confounders. We constructed sex specific models as follows. A linear term for age was always considered. Sensitivity analyses showed that a squared age term was not significant in most models; where it was, the results did not substantially change. Next, comorbidities diagnosed at the index event or in the previous three years were considered in the model for angioplasty use. However, when examining short term mortality, only comorbidities diagnosed in prior hospitalisations were included. This approach served to avoid coding bias, namely the apparent “protective effect” of certain less severe diagnoses (for example, hypertension) because of the tendency to omit these diagnoses for severely ill patients.18 For longer term outcomes (fatality, hospital readmissions for AMI or for other cardiac causes within one year) all comorbidities diagnosed either at the index event or previously were considered, as was PTCA at the index hospitalisation. All models were reduced to exclude comorbidities not associated with the outcome (p>0.20). In subsequent overall analyses of both sexes, interaction terms between sexes and comorbidities were included when relevant.
RESULTS
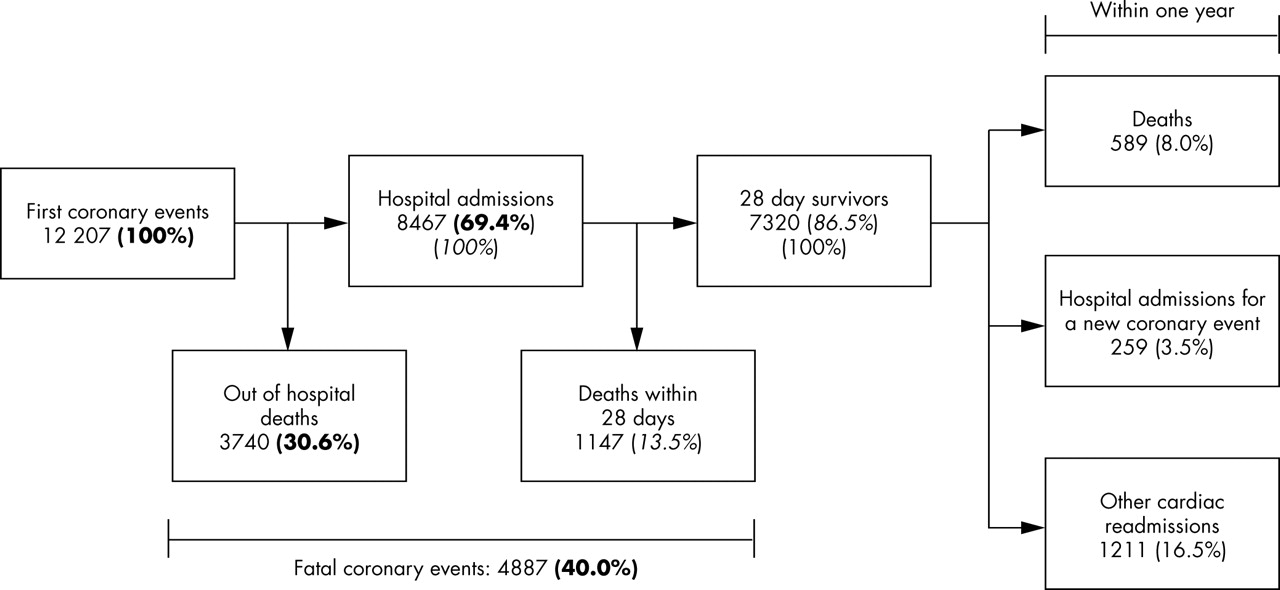
In all, 12 207 coronary events (3740 out of hospital deaths and 8467 hospitalisations) were found in the Rome population between 35 and 84 years old over the three year period. Figure 1 summarises the short term and one year outcomes. Ischaemic heart disease (ICD-9: 410–414) accounted for slightly more than half of the deaths of the 589 (8.0%) 28 day survivors who died within a year of their first coronary event.
{kind=link}
First coronary events and their outcomes in the population of Rome, age 35–84 years, 1998–2000.
Table 1 shows the distribution of total cases, out of hospital deaths, and hospitalised cases according to gender, age, area based deprivation status, and comorbidities diagnosed in the three preceding years, and, for the hospitalised patients, educational attainment. People who died out of hospital were more likely to be older and female than those hospitalised for AMI. Area based deprivation status was available for 94.5% of the study subjects, while educational attainment was available for 85.4% of hospitalised patients.
Descriptive characteristics of residents of Rome (aged 35–84 years) who had a first coronary event during the period 1998–2000
Table 2 reports sex specific age standardised incidence rates and relative risks of first coronary event by deprivation status. A clear trend was evident: the more deprived groups experienced higher rates and had relative risks significantly greater than 1.0 relative to the most privileged group. The socioeconomic gradient was more pronounced for hospitalisations (RR = 1.42 men, 2.04 women lowest compared with highest) than for out of hospital deaths (RR = 1.36 men, 1.35 women). The interaction of gender with deprivation status was significant for hospitalisations (p<0.05).
Area based deprivation status and incidence of first coronary events in Rome, 1998–2000: age standardised annual rates (per 100000 residents), age adjusted relative risks and confidence intervals (95% CI)
Table 3 reports the frequency distribution of comorbidities in the three years before AMI hospitalisation and at the index event for the four deprivation categories. Although no differences were observed for most comorbidities considered, three diseases were more represented in the less privileged group at the index event: diabetes, COPD, and arrhythmias. Deprived patients were also more likely to have suffered diabetes, hypertension, COPD, and heart failure in the preceding three years.
Frequency distribution (%) of comorbidities diagnosed in the preceding three years, and secondary diagnoses at the index AMI hospitalisation, by area based deprivation status among hospitalised patients aged 35–84 years in Rome, 1998–2000
Table 4 displays crude absolute risks, adjusted odds ratios for the outcomes in the hospitalised group, and adjusted hazard ratios for one year follow up outcomes in the 28 day survivors. In total, 789 hospitalised patients (9.3%) received PTCA at their index hospitalisation. As area based deprivation increased, the likelihood of receiving PTCA decreased (p for trend 0.02). The trend was clearer for men than for women, but significantly lower PTCA rates were seen for women than for men (OR = 0.53, 95% CI: 0.40, 0.72).
Association between neighbourhood based SES and outcome of first AMI hospitalisation in Rome, 1998–2000
Overall, area based deprivation status was not significantly associated with other outcomes, although a tendency of higher short term mortality for more deprived groups was suggested for women (p for trend 0.05). No effect modification by sex was found for the one year outcomes.
Agreement between area based deprivation status and individual educational attainment was high. The proportions of patients with at least a high school diploma were 32.3% and 16.2% in the most and least affluent census blocks, respectively, while 25.4% and 38.1%, respectively, had not completed middle school (p for trend<0.01).
Table 5 gives results of analyses using individual educational attainment as the exposure variable. The least educated patients were least likely to receive PTCA (p for trend, 0.004), especially among men. Crude fatality rates (both short term and first year) seem to show disparities, but strong confounding by age was present. Indeed, educational attainment was strongly correlated with age (p for trend <0.01): 15% of patients aged 75–84 years had at least a high school diploma, compared with 53% of those aged 35–44. Hence, the age adjusted odds ratios for short term mortality were smaller than expected and not statistically significant in the gender stratified analyses. Overall, however, a small effect of educational attainment on short term, but not first year, mortality remained (OR = 1.24, p for trend 0.04). No other educational disparities reached statistical significance, and gender did not modify the effect except in the case of PTCA.
Association between level of education attained and outcome of first AMI hospitalisation in Rome, 1998–2000
DISCUSSION
Three MONICA studies found rates of out of hospital deaths among lower SES strata19: one included only men,2 one found equal effects of SES among women and men,1 and one found weaker effects of SES among women,3 but all examined a restricted age range where women rarely suffer coronary events. A Scottish study found that the social deprivation gradient was less steep among women than among men.20 In Rome, the relative risk (most compared with least deprived areas) of out of hospital death was about equal for men and for women.
However, the socioeconomic gradient in the hospitalisation rate for AMI in the Rome population was much steeper for women than for men. Previous results on this outcome are sparse, but total incidence has been studied. In Finland, those of lower income or education level had higher total incidence rates among both sexes, with effect modification by gender depending on which measure was used.3 In Scotland, as in Rome, overall incidence had a strong socioeconomic gradient that was steeper for women than for men.1 In the USA, the steeper educational gradient for women than for men in total incidence of coronary heart disease was mainly attributable to body mass index.21 However, in all cases, SES accounted for more coronary events among men than among women because women’s absolute risk was much lower.
Our negative findings for one year outcomes are consistent with a London study, where only short term mortality rates were higher among more deprived patients.10 This latter disparity was inconsistently evidenced in Rome: only among women when using area based deprivation status and only overall when using educational attainment to measure SES. The London study did not present gender stratified results, and in Glasgow, where short term mortality was not associated with SES, no difference was found between the sexes.1 However, in Finland both short and long term mortality were associated with low SES, with greater effects seen among men than among women.3
In Rome the only post-hospitalisation outcome showing a clear socioeconomic gradient was PTCA. Access to PTCA depends on illness severity and comorbidities.22 Diabetes, COPD, and arrhythmia were more prevalent in the most disadvantaged Roman patients, consistent with many studies showing more severe clinical findings in patients of lower SES.6,8,9,19,23 However, this did not explain differential access to PTCA: recanalisation procedures were less likely to be performed on those living in deprived areas, on those with lower educational attainment, and on women, even after adjusting for comorbidities. As PTCA was only just becoming widespread during the years studied, social disparities in receiving this surgery might no longer exist. However, our results are consistent with findings from the USA,8 Canada,6 and Scotland.24 In Canada, geographical proximity to a hospital offering the service did not fully account for differential access to angiography by SES.25 As in Rome, North American women were significantly less likely than men to undergo recanalisation6,26; in Scotland gender differences depended on the procedure.24 In the former Yorkshire Region (UK), socioeconomic inequities in access to revascularisation procedures varied geographically.27 In Finland, such sex and socioeconomic inequities in access decreased from 1988 to 1996, but were not eliminated completely.28 Finally, in Rome, living in a deprived area (same indicator used as in this study) was associated with reduced access to coronary care units.14 Hence, many locations show evidence of treatment disparities, although publication bias may exaggerate such inequality and the causes may not be the same for different treatments and locations.
Some limitations of the study should be mentioned. Deprivation status was area based and may not accurately represent the person’s true SES. However, several studies found that neighbourhood socioeconomic environment had significant effects on coronary heart disease hospitalisations and mortality, even after adjustment for individual level SES measures.29–31 Although the urban structure of Rome is different from that of northern European cities, where segregation by SES is more pronounced, the census blocks used in defining deprivation status were small enough (average population 466) to capture disparities: this indicator is associated to many health outcomes previously studied.14,17,32,33 Deprivation status was also based on 1991 census data, which could be outdated. Resulting misclassifications did not preclude detection of clear differences at the population level but may have masked post-hospitalisation outcomes. Rather consistent results were found, however, when using individual educational attainment.
What this paper adds
The socioeconomic gradient in total incidence of coronary events was steeper among women than among men in Rome, but this was attributable to hospitalisations rather than out of hospital deaths. Area based deprivation status and individual educational attainment seemed not to influence one year prognosis, but were significant predictors of access to PTCA.
We selected the subjects under study based on linkage between various registries and following examples from other countries.34,35 Our definition of out of hospital death for coronary event is consistent with a restricted version of the definition of “possible fatal coronary heart disease” in a 2003 Scientific Statement of the American Heart Association.36 Hospitalisation for AMI was defined as having primary diagnosis ICD-9 = 410, whose accuracy in hospital discharge records in Rome has been previously validated.37,38 As only the first event was considered, our results may not hold for repeated events. When an AMI patient suffers serious complications, these may be reported as the principal diagnosis while AMI is reported as a secondary diagnosis; such patients are more likely to experience adverse short and long term outcomes. Because we excluded these subjects, if they lived in more deprived areas then a bias towards the null could have occurred.
A selection bias based on severity could be responsible for the weak and negative post-hospitalisation findings. If emergency health services were provided disproportionately to wealthier neighbourhoods, then those from deprived areas who reached the hospital would be the ones with less severe AMI. They would therefore have a better prognosis than those from wealthy areas, who would arrive at the hospital even with a more severe AMI. Consequently, differences in treatment or prognosis, favouring higher SES strata, would be underestimated. To evaluate the presence of such a selection bias, we examined the relative proportion of total first coronary events that were out of hospital deaths for each deprivation category (see table 2). Among men, the age adjusted proportion of total first coronary events that were out of hospital deaths was roughly constant across deprivation categories (between 25.9 and 27.7%). However, among women this proportion decreased substantially from 37.3% in the most privileged category to 27.5% in the least. Hence, somewhat counterintuitively, privileged women who suffered severe coronary events were more likely to die before reaching a hospital than deprived women. These findings render an effect of selection bias unlikely.
Policy implications
People involved in health care should be aware of the socioeconomic differences in the occurrence of coronary events. Efforts should be made to offer equal access to PTCA treatment in different socioeconomic groups.
Although we were able to consider several baseline comorbidity factors, both recorded before the AMI and during the actual hospitalisation, the main limitation of using administrative data is the impossibility of considering actual AMI severity, lifestyle risk factors, and treatment adherence.
In conclusion, between 1998 and 2000 the population incidence of first coronary events in Rome was higher among the most deprived groups, and the gradient was more pronounced among women. There is evidence that access to effective invasive treatments (PTCA) was not egalitarian with respect to area based deprivation status and especially educational attainment and gender. Short term mortality results were inconclusive. Overall, SES seemed not to influence one year prognosis.
Acknowledgments
The authors thank Margaret Becker for her writing and editing assistance.
REFERENCES
Footnotes
-
Funding sources: this research was partially funded by the European Union (QLK4-2000-00708: Health Effects of Air Pollution on Susceptible Subpopulations) and the Italian National Institute of Health (ISS) (Project 521C/5-VI: Activation of National Registry of Coronary and Cerebrovascular Events).
-
Competing interests: none declared.
Linked Articles
- In this issue