Incidence and thickness of primary tumours and survival of patients with cutaneous malignant melanoma in relation to socioeconomic status
BMJ 1996; 312 doi: https://doi.org/10.1136/bmj.312.7039.1125 (Published 04 May 1996) Cite this as: BMJ 1996;312:1125
- Rona M MacKie, professor of dermatologya,
- David J Hole, principal epidemiologist, Greater Glasgow Health Boardb
- a Department of Dermatology, University of Glasgow, Glasgow G12 8QQ
- b West of Scotland Cancer Surveillance Unit, Ruchill Hospital, Glasgow
- Correspondence to: Professor MacKie.
- Accepted 24 January 1996
Abstract
Objective: To study incidence of and survival from cutaneous malignant melanoma in relation to socioeconomic status.
Design: Application of Carstairs deprivation score to all malignant melanoma patients diagnosed in a geographically defined area over a 15 year period.
Setting: West of Scotland (area population 2 716 900).
Subjects: 3142 patients first diagnosed with malignant melanoma in the period 1979-93.
Interventions: Surgical excision of primary malignant melanoma with additional treatment as appropriate and follow up until December 1994.
Main outcome measures: Malignant melanoma incidence, primary tumour thickness and five year survival by socioeconomic status
Results: From 1979 to 1993, the age standardised incidence rate for cutaneous malignant melanoma was 9.1/100000 for the most affluent men and 2.4/100000 for the least affluent men and 16.1/100000 and 5.0/100000 respectively for most and least affluent women (P<0.001 for trend in both). The incidence increased steadily over time in both sexes in all socioeconomic groups. Good prognosis tumours (<1.5 mm thick) were most common in the most affluent men and women, and over the study period the proportion of such tumours increased most in the intermediate affluence group (both sexes) and in the least affluent women. Five year disease free survival from melanoma for the sexes combined was 81% for most affluent, 77% for intermediate, and 73% for least affluent groups. Even after adjustment for known prognostic factors of tumour thickness, ulceration, age, and body site of primary melanoma, the more affluent the group, the better the survival.
Conclusion: Although the incidence of cutaneous malignant melanoma is higher among more affluent people, the prognosis is better in this group than for less affluent individuals. Early diagnosis campaigns should be targeted particularly to less affluent men and primary prevention campaigns should emphasise the greater risk in more affluent women.
Key messages
Key messages
Paradoxically, five year disease free survival prospects are better for affluent people
Variations in incidence could be explained by differences in sun exposure related to socio- economic status
Variations in nutrition and possibly immune function by socioeconomic status could explain survival differences
In public education campaigns, deprived men should be targeted to encourage earlier diagnosis
Primary prevention campaigns should be tar- geted to more affluent socioeconomic groups
Introduction
Cutaneous malignant melanoma has been reported to be a disease of those in higher paid occupations.1 2 This could relate to differences in exposure to the sun and to affluence: short intense episodes of burning sun exposure, as occur on foreign holidays, are currently believed to be important in the development of malignant melanoma.3
No analysis has been yet been made of melanoma survival by socioeconomic status with control for important predictors of prognosis such as age, sex, ulceration, and tumour thickness of the primary melanoma at the time of initial surgery.4 We carried out such an analysis, looking at all patients presenting with malignant melanoma over a 15 year period in the west of Scotland where there is available, as a result of the activities of the Scottish Melanoma Group, detailed information on clinical and pathological details of all patients presenting with cutaneous melanoma in this area (population 2 716 900). In addition, each patient's postcode enables an area based classification of their socioeconomic status to be made. Throughout the west of Scotland area, groups of very different socioeconomic status experience the same daily climatic conditions, living within 2-3 km of each other.
Methods
Details of melanoma patients were drawn from the records of the west of Scotland section of the Scottish Melanoma Group, which records details of all patients presenting with primary cutaneous malignant melanoma in Scotland.5 A total of 3142 patients (2008 women and 1134 men) diagnosed as having invasive primary cutaneous malignant melanoma (level 2 or deeper) between 1979 and 1993 were identified and were allocated an economic grouping by using the method of Carstairs and Morris.6 This classifies areas according to four measures derived from census data: unemployment, car ownership, overcrowding, and percentages of households where the occupation of its head is classified as social class IV and V. Thus, given a postcode sector of residence, it is possible to allocate a person to one of seven categories from 1, the most affluent, to 7, the most deprived. All deaths up to December 1994 were recorded.
STATISTICAL METHODS
We examined trends in incidence across deprivation categories, comparing observed and expected numbers of cases and applying the χ2 test for trend. Expected numbers of cases for each affluence category were calculated by applying the overall incidence rates for each age group, sex, and year of diagnosis to the appropriate age-sex distribution for each deprivation category for each year of the study; data were then aggregated. Trends in incidence over time were assessed by fitting linear regressions of age standardised rates on year of diagnosis for the affluence-sex subgroups. The gradients derived from the regression models represent average annual increases in rates and were tested statistically, assuming a t distribution.
Dates of death were obtained through contact with the patient's general practitioner and with the registrar general for Scotland through linkage with the west of Scotland cancer registry. Deaths due to melanoma were identified.
The trend in disease free survival across deprivation categories for the different age and sex groups was tested using the log rank statistic.7 Calculation of hazard ratios, to compare disease free survival between affluence categories while allowing for the major recognised prognostic factors (tumour thickness, ulceration, etc), was carried out using Cox's proportional hazards model.8 All variables included in the model were entered as categorical variables with stage at presentation with melanoma in six categories: primary melanoma <1.5 mm, 1.5-2.49 mm, 2.5-3.49 mm, 3.5-4.99 mm, >5 mm thick, and melanoma spread beyond the primary site.
Results
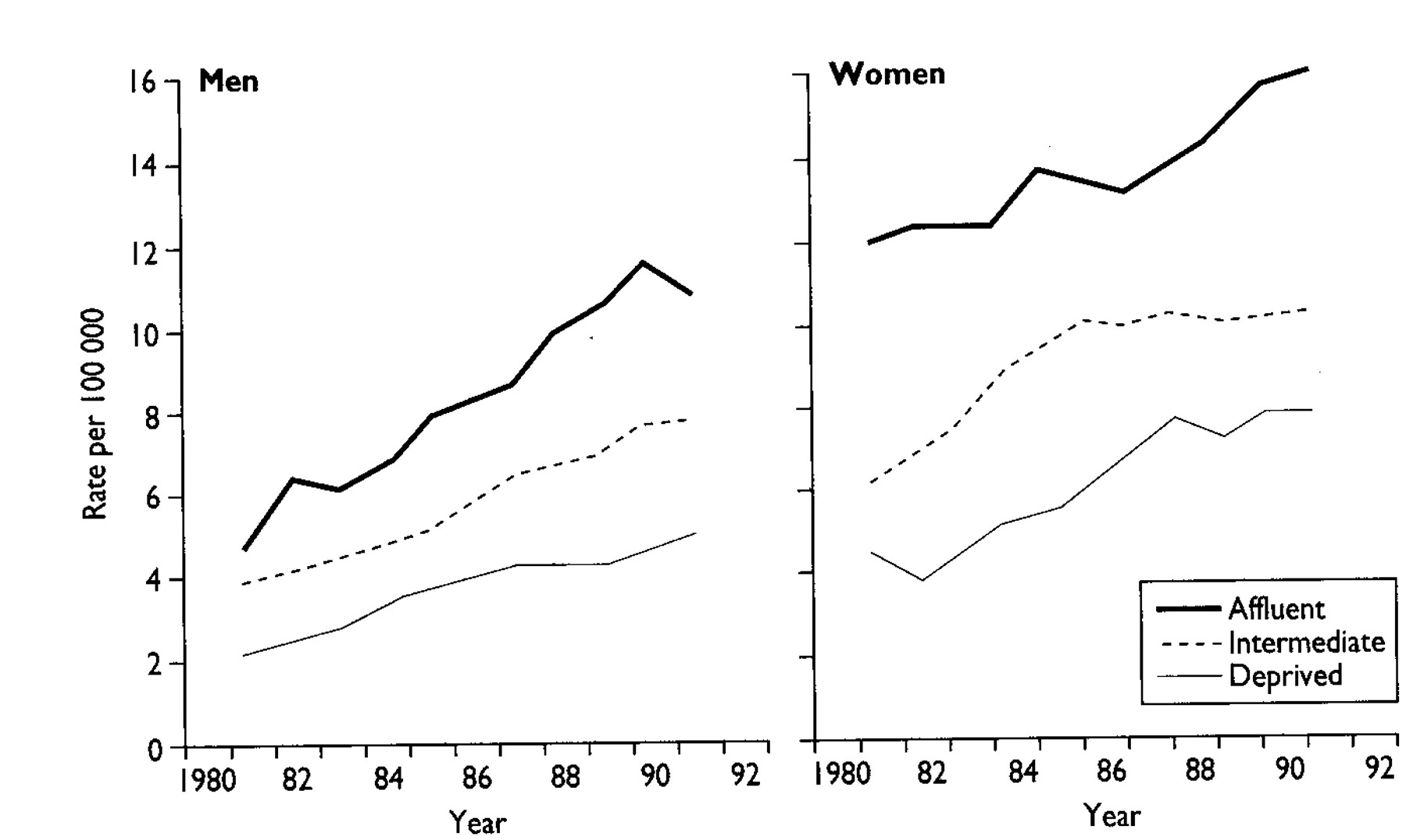
Table 1 presents the average annual age standardised incidence by deprivation category over the 15 year period 1979-93. For both sexes there was a strong (P<0.001) trend in incidence ranging from 2.4/100000 for least affluent men to 9.1/100000 for most affluent men and from 5.0/100000 for least affluent women to 16.1/100000 for most affluent women. Figure 1 shows that for all six subsets—men and women in most affluent, intermediate, and least affluent circumstances—there was a steady increase in incidence over the 15 years studied. The slopes of the six curves are similar, implying that the factors responsible for the rising incidence are acting in all six groups.
Age standardised incidence rates of melanoma by socioeconomic category for men and women; based on cases diagnosed 1979-93

Incidence of melanoma (five year moving averages) in men and women in affluent, intermediate, and deprived categories, 1979-93
{kind=link}
Figure 1 and table 1 also show the clear difference in incidence of malignant melanoma between the sexes, with a female:male ratio of 3:2. This relative over-representation of women is maintained across the socioeconomic spectrum.
Table 2 lists the percentage of patients presenting with tumours less than 1.5 mm thick divided by socioeconomic status and over time. For men in the affluent and intermediate categories, there has been a significant increase in the proportion presenting with thin melanomas between 1979-84 and 1991-3. The highest proportion of thin melanomas in men was seen in the affluent group (61%) in the period 1985-90. For women, the overall trends are similar, and there have been significant increases over time in the proportion of thin tumours in the intermediate and least affluent groups of women. Affluent women had a significantly higher proportion of thin tumours than affluent men (52% v 34%) during the 1979-84 period. As with men, the highest proportion of thin tumours in women (61%) was seen in the most affluent group in the 1985-90 period. In all groups except the least affluent men, the proportion of primary melanomas <1.5 mm at excision is now over 54%.
Percentage (number) of patients presenting with primary melanoma <1.5 mm thick by socioeconomic category over time*
Table 3 and figure 2 show the relation between five year survival and socioeconomic status. For the most affluent men, five year survival is 74% and for the most affluent women it is 84%, compared with 68% and 82% for the intermediate men and women and 61% and 79% for least affluent men and women. The difference in survival between the most affluent group and the other groups was significant (P for trend <0.001), as was the difference in survival between the most affluent men and woment (P<0.001).
Five year survival by socioeconomic category, sex, and age group

Kaplan-Meier survival curves for men and women in affluent, intermediate, and least affluent groups. Only deaths related to melanoma were included for analysis
{kind=link}
Table 3 further divides five year survival by affluence and by age group. In the most affluent groups the five year survival for younger people was 91% while in the least affluent group it was 80% (P=0.04). In people aged 55-64, survival was better in the more affluent groups (P<0.001).
The relative hazard ratios for patients under 65 years presenting with melanoma are shown in table 4. After adjustment for all known prognostic factors such as age, sex, site, ulceration, and primary tumour thickness, the most affluent patients continued to have a survival advantage over the intermediate group, which in return had a better survival than the least affluent group (P for trend <0.001).
Relative hazard ratios derived from Cox's proportional hazards model for survival differences between socio- economic categories for melanoma patients under 65 years of age. Based on 450 deaths among 2008 patients
Discussion
This study is the first to show a relation between thickness at presentation and socioeconomic status, and also the first to relate socioeconomic status to survival. It shows that affluent individuals have more favourable five year survival prospects. Even after the major prognostic factors (tumour thickness, ulceration, age at diagnosis, and site of primary tumour) were controlled for, this difference remained significant. Tumour thickness is commonly regarded as a measure of early diagnosis; when patients were matched for tumour thickness, socioeconomic status continued to be a factor influencing survival. This suggests that a greater knowledge of the features of early melanoma in the affluent group, leading to earlier self referral and thus earlier diagnosis and treatment, does not wholly explain our results.
Recent results from the same geographic area also showed poorer survival for the less affluent patients with breast cancer.9 We speculate that a common factor, such as poor nutrition leading to low levels of antioxidants, or immunological defects, could be responsible in both tumour types.
The pattern of higher incidence but better survival for the most affluent compared with the least affluent of both sexes is mirrored in the greater incidence of melanoma but better survival in women. The greatest risk of developing melanoma is seen in affluent women, and the poorest five year disease free survival prospects in deprived men. It is possible that behavioural differences with regard to sun exposure between the sexes and between affluent and deprived individuals may explain some of the differences in incidence, but this would not explain the differences in survival.
Table 2 shows clearly that over the three time periods studied the proportion of thin tumours has increased in all groups, and that this increase is significant in intermediate and deprived women and affluent and intermediate men. Over 50% of all tumours are now <1.5 mm thick, but among deprived men the proportion is only 39%, indicating that early detection activities need to be targeted particularly at less affluent men.
Footnotes
-
Funding The Scottish Melanoma Group has been funded by the Cancer Research Campaign and is currently funded by the Scottish Home and Health Department.
-
Conflict of interest None.