PapersTwins and maternal smoking: ordeals for the fetal origins hypothesis? A cohort study
BMJ 1999; 318 doi: https://doi.org/10.1136/bmj.318.7188.897 (Published 03 April 1999) Cite this as: BMJ 1999;318:897
Four papers appear in the print BMJ this week in abridged form. The full and abridged versions are both available here on our website. The editorial by Delamothe et al explains why we are doing this, and we welcome readers' reactions. The paper by Whitehead (p.908) appears in two abridged versions, one much shorter than the other; again we welcome readers' reactions on which they prefer, and why.
Twins and maternal smoking: ordeals for the fetal origins hypothesis? A cohort study
- Sheila Williams, senior research fellow (sheila.williams{at}stonebow.otago.ac.nz)a,
- Richie Poulton, senior research fellowb
- Correspondence to: Ms Williams
Abstract
Objective: To assess the direct and indirect effects of being a twin, maternal smoking, birth weight, and mother's height on blood pressure at ages 9 and 18 years.
Design:Longitudinal study.
Subjects: Cohort born in 1972-3.
Setting: Dunedin, New Zealand.
Main outcome measure: Blood pressure at ages 9 and 18 years.
Results: Compared with singletons, twins had a systolic blood pressure 4.55 (95% confidence interval 1.57 to 7.52) mm Hg lower at age 9 after adjustment for direct and indirect effects of sex, maternal smoking, mother's height, socioeconomic status, and birth weight, as well as concurrent height and body mass index. Blood pressure in children whose mothers had smoked during pregnancy was 1.54 (0.46 to 2.62) mm Hg higher than in those whose mothers did not. The total effect of birth weight on systolic blood pressure at age 9 was—0.78 —1.76 to 0.20) mm Hg and that for mother's height was 0.10 (0.06 to 0.14) mm Hg. Similar results were obtained for systolic blood pressure at age 18. The total effect of twins, maternal smoking, and birth weight on diastolic blood pressure was not significant at either age.
Conclusions: Twins had lower birth weight and lower systolic blood pressure at ages 9 and 18 than singletons. This finding challenges the fetal origins hypothesis. The effect of maternal smoking was consistent with the fetal origin hypothesis in that the infants of smokers were smaller and had higher blood pressure at both ages. This may be explained by pharmacological rather than nutritional effects. The total effect of birth weight on systolic blood pressure, after its indirect effect working through concurrent measures of height and body mass index was taken into account, was small.
Editorial by Delamothe et al
Key message
Twins have lower systolic blood pressure at age 9 and 18 years than singletons
Children of mothers who smoke in pregnancy have a lower mean birth weight and a higher mean systolic blood pressure at age 9 and 18.
When the indirect effects of birth weight on current height and body mass index are taken into account the effect of birth weight on bloodpressure is small at ages 9 and 18
Introduction
Studies reporting an inverse association between birth weight and blood pressure in both children and adults have led to the hypothesis that events occurring before birth may lead to cardiovascular disease in later life. 1 2 It is argued that this is the consequence ofthe mother's poor nutrition in pregnancy. Although not all findings confirm this hypothesis,3–5support comes from several studies of people born in the 1920s and 1930s and from children born more recently. The evidence, as aBMJ editorial puts it, is an inductionist's dream; example being pile on example, with each study being somewhat consistent with others but none seriously testing the hypothesis.6 This editorial suggests ordeals or tests to which the hypothesis might be put, including the effect of being a twin, a group known to experienerestricted growth in the third trimester of pregnancy;smoking by the mother, which is akey determinant of birth weight and smoking in the offspring; and social class both at the time of birth and in the mother's family.
This sample from New Zealand provided an opportunity to re-examine the association between birth weight and later blood pressure. Information was available on mothers' height, which can be regarded as a measure of the socioeconomic climate of their childhood as well as the socioeconomic climate prevailing at the time of the children's birth.
Methods
The sample consisted of children enrolled in the Dunedin multidisciplinary health and development study. This cohort was born at Dunedin's only obstetric hospital between 1 April 1972 and 31 March 1973. Their mothers were resident in the Dunedin metropolitanarea at the time of the children's birth.
The sample was traced at the time of the children's third birthdays, and consent wasgiven for 1037 of the 1139 still living in Dunedin or Otago to take part. The sample was seen at intervals of 2 years between ages 3 and 15 and again at ages 18 and 21.7 The present study uses data collected at age 9, when 818 children attended the research unit for physical measurements and their mothers were asked about smoking in pregnancy, and at age 18, when 879 attended the unit for a full day's assessment.
In each phase of the study, the same instruments were used for all participants. Blood pressure was measured using a London School of Hygiene blind mercury sphygmomanometer. Systolic blood pressure was taken as the first Korotkoff sound and diastolic as the fourth. Blood pressure was based on the mean of three measures at age 9 and two at age 18 taken in the recumbent position. Stature was measured to the nearest millimetre with a portable Harpenden stadiometer. Weight was recorded to the nearest 0.1 kg with a Lindell beam balance, the participants being weighed in light clothing. Body mass index was calculated as weight/height2 with units kg/m2. The measurement of blood pressure was one of a number of different assessments undertaken by the participants and was not always completed because of time constraints.
This cohort was part of a larger study in which details of both antenatal and perinatal events were recorded for babies born at Queen Mary Hospital for a period from 1967 to 1973.8BIRTH WEIGHT and mother's height were derived from this. Socioeconomic status for the infants' fathers was recorded, using the Elley-Irving index of socioeconomic status9;children whose fathers had occupations in the semiskilled and unskilled categories (5 and 6) were defined as low socioeconomic status, and children of mothers who were unmarried were assigned to another category. Where data were missing for socioeconomic status the mother's socioeconomic status recorded at the birth or socioeconomic status collected at age 3 was substituted.
As part of the assessment at age 9 the mothers of the children were asked whether or not they had smoked in pregnancy and were classified as smokers or non-smokers. Mother's height was recorded at assessment at age 11, and this was used if mother's height had not been recorded at the time of the child's birth.
Path analysis was used to examine the effect of maternal smoking, mother's height, and being a twin on birth weight as well as their effect on later height, body mass index, and blood pressure. The models were fitted with LISREL using maximum likelihood methods.10 In the analysis, the temporal nature of the variables was used to examine the causal relations among them. As the mother's height was established and maternal smoking occurred before the baby was born, these variables were regarded as being causally related to birth weight. Birth weight was considered to be causally related to measures taken at ages 9 and 18 years. Although height, body mass index, and blood pressure were collected simultaneously, a causal relation between both body mass index and height and blood pressure was tenable. This mediates the direct and indirect effects of birth weight and other variables on blood pressure.
Results
Systolic blood pressure was recorded for 811 children at age 9 but the analysis was restricted to 419 boys and 376 girls because data for some of the other variables were missing (see below). The means and standard deviations for systolic blood pressure, height, body mass index, birth weight, and mother's height are shown in table 1. The sample included 22 (2.8%) twins and 261 (32.8%) children whose mothers reported smoking in pregnancy. Information on whether or not the mothers smoked was not available for 40 (5.0%) children. The sample also included 177 (22.3%) children in the low socioeconomic status category and 36 (4.5%) whose mothers were unmarried at the time of their conception. Height and weight at age 9 were missing for five children, mother's height for two, and socioeconomic status for nine. The mean birth weight for the 242 children not included in this study was 3.35 (SD 0.50) kg compared with 3.38 (0.53) kg for those included. The mean of the mothers' heights was 163.0 (6.58) cm for children who were excluded and 162.9 (5.84) cm for those included. Of those excluded 125 (51.7%) were boys, 4 (1.6%) were twins, 53 (21.9%) were categorised as of low socioeconomic status, and 6 (2.5%) had single mothers.
Characteristics of males and females at age 9 and 18 years. Values are means (SD)
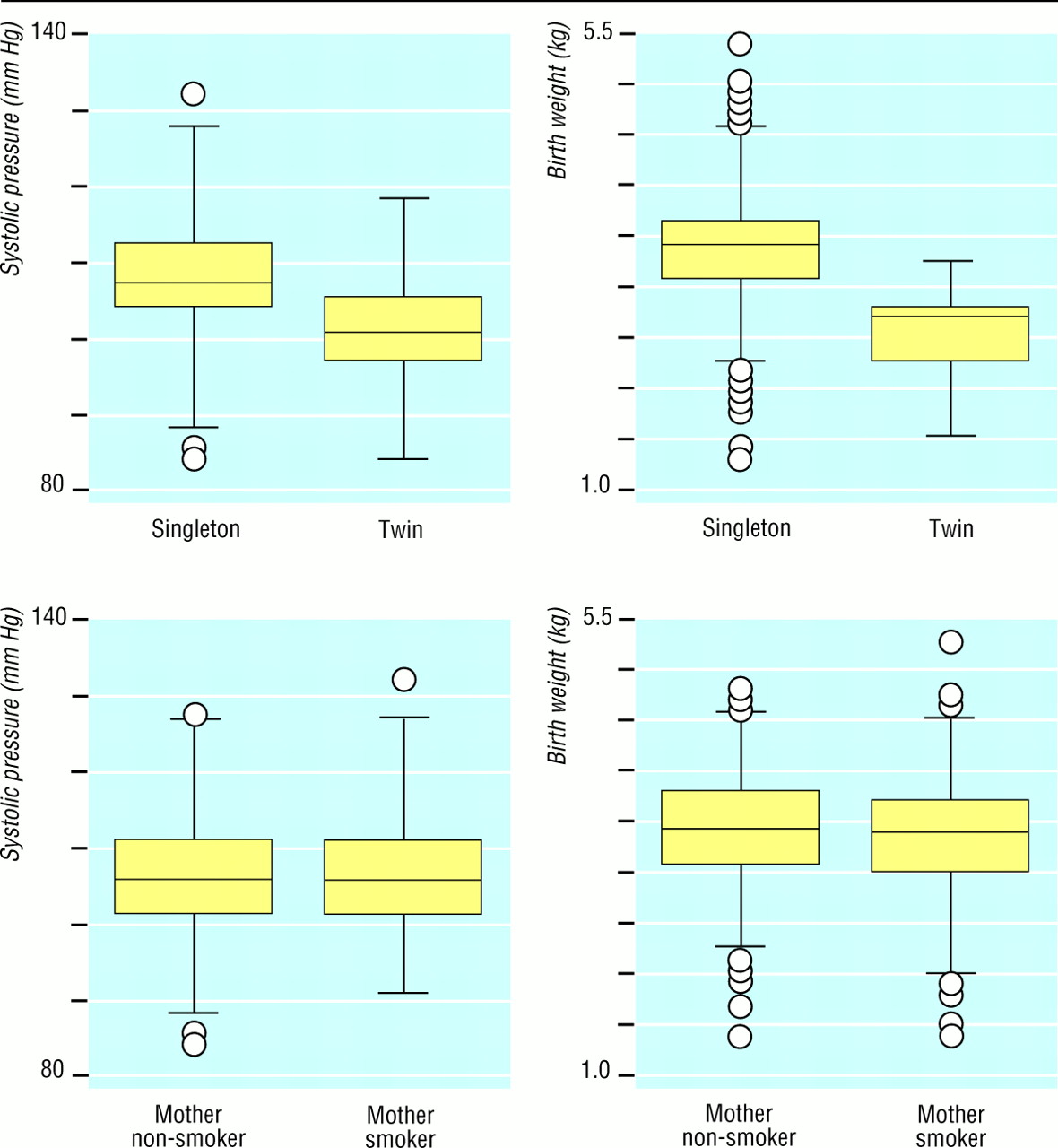
Box and whisker plots for systolic blood pressure and birth weight for single and twin births, and for children whose mothers were and were not smokers, are shown in figure 3. These indicate that on average twins had both lower blood pressure at age 9 and lower birth weights than singleton children (difference 5.09 (95% confidence interval 2.03 to 8.16) mm Hg for blood pressure and 0.88 (0.66 to 1.09) kg for birth weight). The children of mothers who smoked in pregnancy had higher blood pressure (difference 1.41 (0.32 to 2.50) mm Hg) and lower birth weights (difference 0.11 (0.03 to 0.19) kg) than those whose mothers did not smoke.

Box and whisker plots for systolic blood pressure at age 9 and birth weight for twins compared with singletons, and children of mothers who smoked during pregnancy compared with children of mothers who did not smoke
{kind=link}
Regressing systolic blood pressure on birth weight in the total population of birthsshowed an inverse relation: a difference of 1 kg in birth weight was commensurate with a decrease in blood pressure of 0.26 (0.70 to 1.21) mm Hg. Mother's height was positively related, with a difference of 1 cm being commensurate with a difference of 0.07 −0.02 to 0.15) mm Hg. The results of regressing systolic blood pressure at age 9 on all the variables simultaneously is shown in table 2. These are the direct effects of each variable on blood pressure. Being a twin, maternal smoking, the concurrent measures of body mass index and height, as well as birth weight, were all significantly associated with blood pressure. Birth weight was inversely associated with blood pressure, commensurate with a decrease of 1.93 (0.96, 2.89) mm Hg for each kg increase in birth weight. This analysis, however, does not take into account the indirect effects of a number of these variables on blood pressure.
Regression coefficients for effects of predictors of systolic blood pressure at age 9 adjusted for other variables in model
Path analysis was used to estimate both the indirect and the total effects of the measures related to birth weight as well as birth weight itself on the height, body mass index, and blood pressure at age 9 (table 2). As the path model estimated a large number of effects, in the interests of parsimony the direct effects which were not statistically significant were removed. The final model provided a good fit for the data χ2=14.07, df=11, P=0.23) The key features of the model are illustrated in figure 2, which shows the standardised regression coefficients. Being male, being a twin, and mother's height were strong predictors of birth weight and later height. Maternal smoking was related to birth weight and later body mass index. In this model the total effect of birth weight on systolic blood pressure included the direct effect, −0.134; the indirect effect acting through height, 0.163£0.247; and the indirect effect acting through body mass index, 0.179£0.207; leading to total of −0.057. Thus an increase of one standard deviation in birth weight was associated with a reduction of 0.057 of a standard deviation of systolic blood pressure, which is equivalent to a 1 kg increase in birth weight, being commensurate with a decrease of 0.78 −0.20 to 1.76) mm Hg in blood pressure. The direct effect, and indirect effects operating through birth weight and height, produce a total effect for being a twin of−4.55 −7.52 to −1.57) mm Hg. The total effect for maternal smoking was 1.54 (0.46 to 2.62) mm Hg, and that for mother's height 0.10 (0.06 to 0.14) mm Hg. The correlation between height and body mass index at age 9 was 0.14. The total effects for the full model are shown in table 2.

Path diagram for effects of sex, being a twin, mother's smoking, and mother's height on birth weight, and their effects on height, body mass index, and systolic blood pressure at age 9 years
{kind=link}
We then restricted the analysis for systolic blood pressure at age 9 to the 755 children whose gestational age was believed to be 37 weeks or more. This group included 94 children of unknown gestational age whose mean birth weight was 3.4 (0.46) kg. Nine children whose gestational age was unknown and who were of low birth weight were excluded. The findings were essentially the same as for the entire sample. The total effect on blood pressure was −0.49 −1.62 to 0.64) mm Hg for birth weight,−4.26 −7.75 to −0.77) mm Hg for being a twin, 1.61 (0.50 to 2.73) mm Hg for maternal smoking, and 0.11 (0.07 to 0.14) mm Hg for mother's height (table 3).
Total effects of birth weight, being a twin, maternal smoking, and mother's height on systolic and diastolic blood pressure at age 9 and 18
When the model presented in figure 2 was fitted to the data for diastolic blood pressure at age 9 (table 1) the total effect of birth weight on blood pressure was−0.10 (−1.04 to 0.84) mm Hg, that for being a twin was −1.74−(4.57 to 1.08) mm Hg, that for maternal smoking was 0.54 (−0.49 to 1.57) mm Hg, and the effect for the mother's height was 0.03 (−0.01 to 0.05) mm Hg.
The analysis was repeated using blood pressure measures obtained at age 18. Systolicblood pressure was available for 851 people at this age. Means and standard deviations for blood pressure and the other variables included in the analysis are shown in table 1. Observations were available for 21 (2.5%) twins, 237 (27.8%) participants whose mothers smoked, and 189 (22.2%) whose families were of low socioeconomicstatus. The model shown in figure 2was modified by including a direct path from sex to systolic blood pressure, and the path from maternal smoking to current body mass index was excluded because these results were not significant. The total effects on blood pressure were similar to those observed at age 9. They were −1.17 (−2.41 to 0.06) mm Hg for birth weight, −4.18(−8.12 to −0.24) mm Hg for twins, 1.95 (0.54 to 3.36) mm Hg for maternal smoking, and 0.11 (0.06 to 0.16) mm Hg for mother's height.
Fitting the model for diastolic blood pressure at age 18 led to the following estimates: birth weight 1.03 (0.31 to 2.38) mm Hg, twins 1.19 (−3.10 to 5.49), maternal smoking 1.15 (−0.42 to 2.72), and maternal height 0.05 (0 to 0.11).
Discussion
The significant inverse association between birth weight and systolic blood pressure after adjustment for current height and body mass index at ages 9 and 18 is consistent with the results of a number of studies in both adults and children, several of which are summarised by Barker.2 Our results are not altogether consistent with a more recent study of 8-11 year old children, which found that this association held for girls but not boys,11 nor with a study of 18 year olds in Israel, which found a weak association.3 It has been argued that body mass index is an intervening variable in the relation between birth weight and blood pressure and that to adjust for it in a regression model is to overcontrol for it.6Thus, and because birth weight was not by itself significantly associated with blood pressure in this sample, its importance in the model may be by virtue of its association with other variables.
Statistical considerations
The direct effects in the path analysis were the same as those obtained from multiple regression, so that the measurement for birth weight provided an estimate of its effect on blood pressure after the effects of other variables were taken into account. Adjusting for confounding in this way assumes that none of the variables included in the model are at an intermediate step in the causal pathway. Path analysis, unlike multiple regression analysis, allows for the inclusion in the model of variables such as current height and body mass index which are in the causal pathway. Hence the total effect of birth weight on blood pressure can be estimated from the direct and the indirect effects. The results of this study showed that birth weight was strongly associated with later height and body mass index, which were in turn strongly associated with blood pressure. This resulted in a significant positive indirect effect and, combined with the inverse direct effect, provided an estimate of the total effect.
Ordeals for the fetal origins hypothesis
The most interesting finding of this study was the lower systolic blood pressure of twins. The magnitude of this effect was similar whether or not adjustments were made for birth weight or concurrent height or body mass index. Further, this finding was significant when the analysis was restricted to full term infants at age 9 and when the whole sample was examined at age 18. This finding is not consistent with the fetal origins hypothesis, which argues that poor nutrition in pregnancy leads to higher rather than lower blood pressure. A recent Danish study showed that twins do not have significantly different mortality from cardiovascular disease than the general population, even though they experience intrauterine growth delay.12 The authors concluded that the fetal origins hypothesis did not apply to the growth retardation experienced by twins. Other studies have found that variables plausibly reflecting poor maternal nutrition, including low maternal body mass index before pregnancy, poor maternal weight gain in pregnancy, and being born small for gestational age, were not associated with higher blood pressure.13
The path analysis showed that mother's height had a positive effect on blood pressure, acting indirectly through children's height. Studies that have shown the reverse have not taken into account the indirect effect of maternal height. A study of the British 1946 birth cohort, for example, showed that the 36 year old sons of the tallest mothers had blood pressures 2 mm Hg lower than the sons of the shortest mothers, and this increased to almost 3 mm Hg when adjusted for current weight.14The differences were not as clear cut among the women. This effect was also evident among children born in Salisbury in 1984-5.15The authors of these reports argue that a woman's physique depends on her nutrition in childhood, and that this may be linked to blood pressure in the next generation. In our sample a difference in height of 10 cm was commensurate with a 1 mm Hg difference in blood pressure.
The model in figure 2 showed that maternal smoking worked in three plausible ways. In some senses this finding is consistent with the fetal origins hypothesis in that maternal smoking was associated with both lower birth weight and higher blood pressure if it is assumed that maternal smoking leads to poorer nutrition for the fetus. As smoking also predicts body mass index at age 9 it seems possible that this is an effect of social environment because it is well known that maternal smoking is associated with low socioeconomic status and lower school achievement and may be a proxy for a poorer home environment or poorer nutrition.16 Indeed, a study of the mothers of these children carried out in 1994 found that those who smoked met fewer of the New Zealand nutritional guidelines.17 It also seems possible that smoking has non-nutritional effects that exert a direct effect on the fetus and that this may be mediated by an effect on the placental circulation.16Another study has examined the association between maternal smoking and blood pressure and shown non-significant differences of about 1 mm Hg in blood pressure between the 4 year old children of mothers who smoked 20 or more cigarettes a day and those of mothers who did not smoke in pregnancy.15The authors concluded that although smoking was associated with reduced placental weight it was not related to children's blood pressure. The result in this report could be affected by recall bias because information about smoking in pregnancy was collected after a nine year interval; however, its effects on birth weight are consistent with what is known and it is likely that women remember whether or not they smoked in pregnancy. Studies have shown that people may have difficulty recalling how much they smoked rather than whether or not they smoked.18The finding that the path between maternal smoking and body mass index at age 18 was not significant may mean that the family social environment was less influential at that age.
Conclusions
The fetal origins hypothesis has been subjected to as tough an ordeal as the data permit. The crucial tests were the effects of being a twin and maternal smoking on the relation with systolic blood pressure. That twins had lower blood pressure at age 9 and 18 challenges the underlying premise of the fetal origin hypothesis. On the other hand, smoking affects both birth weight and blood pressure itself and the associations were consistent with the fetal origins hypothesis provided that its action is explained by poor nutrition. Taken in total, mother's height had a positive effect on blood pressure, suggesting that taller women had larger babies, taller children, and children with higher blood pressure. When the indirect effect of birth weight on current height and body mass index was taken into account, it seems that the direct effect of birth weight on later blood pressure may be overestimated.
Acknowledgments
We thank Professor Jim Mann, with whom this paper was discussed, and acknowledge the support of Dr Phil Silva, of those who collected the data, and of the participants who have so willingly taken part in this longitudinal study.
Contributors: SW conceived the idea for this study and carried out the statistical analysis for this study. The paper was written jointly by SW (guarantor) and RP.
Footnotes
-
Funding The Dunedin Multidisciplinary Health and Development Research Unit and the authors are supported by the Health Research Council of New Zealand. The New Zealand National Heart Foundation provided support for the blood pressure studies.
-
Conflict of interest None declared.