Stable partnership and progression to AIDS or death in HIV infected patients receiving highly active antiretroviral therapy: Swiss HIV cohort study
BMJ 2004; 328 doi: https://doi.org/10.1136/bmj.328.7430.15 (Published 01 January 2004) Cite this as: BMJ 2004;328:15
- Jim Young, biostatistician1,
- Geest Sabina De, professor of nursing3,
- Rebecca Spirig, senior research fellow3,
- Markus Flepp, reader in internal medicine4,
- Martin Rickenbach, epidemiologist5,
- Hansjakob Furrer, reader in internal medicine6,
- Enos Bernasconi, head of unit7,
- Bernard Hirschel, professor of infectious diseases8,
- Amalio Telenti, professor of infectious diseases9,
- Pietro Vernazza, reader in internal medicine10,
- Manuel Battegay, professor of infectious diseases2,
- Heiner C Bucher (hbucher{at}uhbs.ch) Swiss HIV Cohort Study Group, professor of clinical epidemiology1
- 1 Basel Institute for Clinical Epidemiology, University Hospital Basel, Hebelstrasse 10, Basle, CH-4031, Switzerland
- 2 Division of infectious Diseases and Hospital Hygiene, University Hospital Basel
- 3 Institute of Nursing Science, University of Basel, Basle
- 4 Division of Infectious Diseases, University of Zurich, Zurich, Switzerland
- 5 Data Centre of the Swiss HIV Cohort Study, University of Lausanne, Lausanne, Switzerland
- 6 Division of Infectious Diseases, University Hospital Berne, Berne, Switzerland
- 7 Ambulattorio malattie infettive, Ospedale Civico, Lugano, Switzerland
- 8 Division des maladies infectieuses, Hôpital Universitaire de Genève, Geneva, Switzerland
- 9 Division des maladies infectieuses, Centre Hospitalier Universitaire Vaudois, Lausanne
- 10 Division of Internal Medicine, Cantonal Hospital Saint Gall, Saint Gall, Switzerland
- Correspondence to: H C Bucher
- Accepted 10 October 2003
Abstract
Objectives To explore the association between a stable partnership and clinical outcome in HIV infected patients receiving highly active antiretroviral therapy (HAART).
Design Prospective cohort study of adults with HIV (Swiss HIV cohort study).
Setting Seven outpatient clinics throughout Switzerland.
Participants The 3736 patients in the cohort who started HAART before 2002 (median age 36 years, 29% female, median follow up 3.6 years).
Main outcome measures Time to AIDS or death (primary endpoint), death alone, increases in CD4 cell count of at least 50 and 100 above baseline, optimal viral suppression (a viral load below 400 copies/ml), and viral rebound.
Results During follow up 2985 (80%) participants reported a stable partnership on at least one occasion. When starting HAART, 52% (545/1042) of participants reported a stable partnership; after five years of follow up 46% (190/412) of participants reported a stable partnership. In an analysis stratified by previous antiretroviral therapy and clinical stage when starting HAART (US Centers for Disease Control and Prevention group A, B, or C), the adjusted hazard ratio for progression to AIDS or death was 0.79 (95% confidence interval 0.63 to 0.98) for participants with a stable partnership compared with those without. Adjusted hazards ratios for other endpoints were 0.59 (0.44 to 0.79) for progression to death, 1.15 (1.06 to 1.24) for an increase in CD4 cells of 100 counts/μl or more, and 1.06 (0.98 to 1.14) for optimal viral suppression.
Conclusions A stable partnership is associated with a slower rate of progression to AIDS or death in HIV infected patients receiving HAART.
Introduction
Cohort studies have shown that social relationships influence mortality. Having fewer close friends or relatives, less frequent contact with other people, and reduced social participation have all been associated with increased mortality, especially in elderly people and in men.1–4 People living alone have a higher mortality from cardiovascular disease and a poorer prognosis after a cardiac event.5 6 However, little is known about the impact of social relationships on outcome for people infected with HIV, most of whom are under 40 years old.
Social support, the emotional or tangible support available from other people, is one of the primary ways in which social relationships influence health.7 In particular, greater emotional support is strongly associated with lower mortality.3 8 Social support may have physiological effects on the neuroendocrine or immune systems.9 10 Poor social support has been linked to a more rapid decrease in CD4 cell counts in HIV infection.11 12 Social support may have psychological effects, such as reducing anxiety and depression.13 Social support may also moderate risk behaviours and improve adherence to treatment.14 15
Little is known about the effect of social support on outcome in HIV infection. Most definitions of social support emphasise family ties or social activities,16 and these may be less relevant for people living with HIV.17 For many people with HIV, a partner may be the most important source of emotional and tangible support. We investigated the association between a stable partnership and disease progression in HIV infected people receiving highly active antiretroviral therapy (HAART).
Methods
Participants
The Swiss HIV cohort study is a prospective cohort study with continuing enrolment of HIV infected patients aged 16 years or over. All participants have given written informed consent. Since 1993, patients enrolled have been asked at visits scheduled every six months whether they have had sexual intercourse with a stable partner during the previous six months. From April 2000 on, this single question was asked as two separate questions (presence of stable partner and sexual intercourse with that partner) as part of a new questionnaire on sexual behaviour.
HAART became available to all residents of Switzerland in August 1996, when its cost was covered by compulsory health insurance. In this analysis, HAART is defined as the combination of at least two reverse transcriptase inhibitors with one boosted or non-boosted protease inhibitor or one non-nucleoside reverse transcriptase inhibitor. As of 28 February 2002, 5350 patients in the cohort had started HAART. We included in our analysis all patients who started HAART and had CD4 lymphocyte counts and plasma HIV RNA (viral load) measured within three months before starting HAART and at least one follow up visit more than one month after starting HAART.
Endpoints
We considered the association between stable partnership and several clinical and surrogate marker endpoints. We selected two clinical endpoints: (a) new US Centers for Disease Control and Prevention (CDC) group C disease18 or death (primary endpoint) and (b) death alone. We also considered four surrogate marker endpoints: (a) increase in CD4 cell count of at least 50 above baseline, (b) increase in CD4 cell count of at least 100 above baseline, (c) optimal viral suppression (a viral load below 400 copies/ml), and (d) viral rebound (the first of two consecutive measurements of more than 400 copies/ml) in patients achieving optimal viral suppression.
Statistical analysis
We estimated the proportion of patients in the cohort reporting a stable partnership since starting HAART. We included patients from their first follow up visit after starting HAART until their latest follow up visit. We assumed that patients reporting a stable partnership remained in a stable partnership until at a subsequent visit they either reported no stable partner or refused to answer the relevant questions. We defined stable partnership as reporting both a stable partner and sexual intercourse with that partner during the previous six months, so as to use a constant definition before and after April 2000.
We used Cox proportional hazards models to estimate the association between a stable partnership and disease progression since starting HAART. Our models included left truncated observations, strata and covariates, and a time dependent treatment variable. Firstly, some patients were registered with the cohort after starting HAART. We included these participants as left truncated observations so that they contributed to estimates only after registration. Secondly, we needed strata within which participants had roughly identical rates of disease progression. We stratified by previous antiretroviral therapy and by clinical stage at baseline (CDC group A, B, or C). This stratification by disease severity at baseline also avoids potential bias if sicker patients are less likely to form stable partnerships because of the severity of their illness.19 Thirdly, we needed to estimate the association between stable partnership and disease progression after adjustment for other variables that might potentially influence the rate of disease progression. We used as covariates CD4 cell counts and viral load at baseline, age and sex, and education and transmission group categories. Fourthly, we represented stable partnership by a time dependent variable to avoid “survivor treatment selection bias,”19 whereby participants who had been followed for longer had had more opportunity to form a stable partnership. In our models “treatment” starts only when a patient first reports a stable partnership. Under the intention to treat principle, treatment then continues for a patient even if the stable partnership ends. This avoids potential bias caused by sicker patients discontinuing a stable partnership because of the severity of their illness.
We used SAS version 8.2 for the analyses. We assessed the evidence for an association between disease progression and another variable by using a hypothesis test based on the difference in the log likelihood ratio between the full model and a reduced model without that variable. We assessed the nature of any association between disease progression and another variable by using a hazard ratio. We give Wald based 95% confidence intervals for all hazard ratios.
Results
Participants
As of 28 February 2002, 5350 patients in the cohort had started HAART. We analysed data from the 3736 (70%) patients who had had CD4 cell counts (4130, 77%) and viral load (4041, 76%) measured within the three months before starting HAART and at least one follow up visit more than one month after starting HAART (5105, 95%). We followed these patients for a total of 12 173 patient years (median 3.6 years per patient).
Patients included in our analysis were on average similar in age, sex, and most likely source of infection (transmission group) to those excluded (table 1). However, those included were more likely to have a higher level of education (more than mandatory schooling), less likely to belong to ethnic groups other than white European, less likely to be in CDC group C, and more likely to have had antiretroviral therapy before starting HAART.
Baseline characteristics for participants in the Swiss HIV cohort study on HAART and those in the analysis who did not reach the primary endpoint. Values are numbers (percentages) unless stated otherwise
When starting HAART, 52% (545/1042) of participants reported a stable partnership. This percentage decreased to around 46% (190/412) after five years of follow up (fig 1a). Beyond five years, estimates of the percentage reporting a stable partnership are unstable because they are based on a small sample; estimates based on a sample size of less than 30 are not shown. The decrease in the percentage reporting a stable partnership over time seems to be related to increasing age. The decrease was obvious among participants aged over 40 (fig 1c). The decrease in the percentage reporting a stable partnership was similar among participants in each of the three clinical stages at baseline (fig 1d). If infection with HIV made it more difficult to maintain a stable partnership, we might expect to see a more rapid decrease among sicker patients.
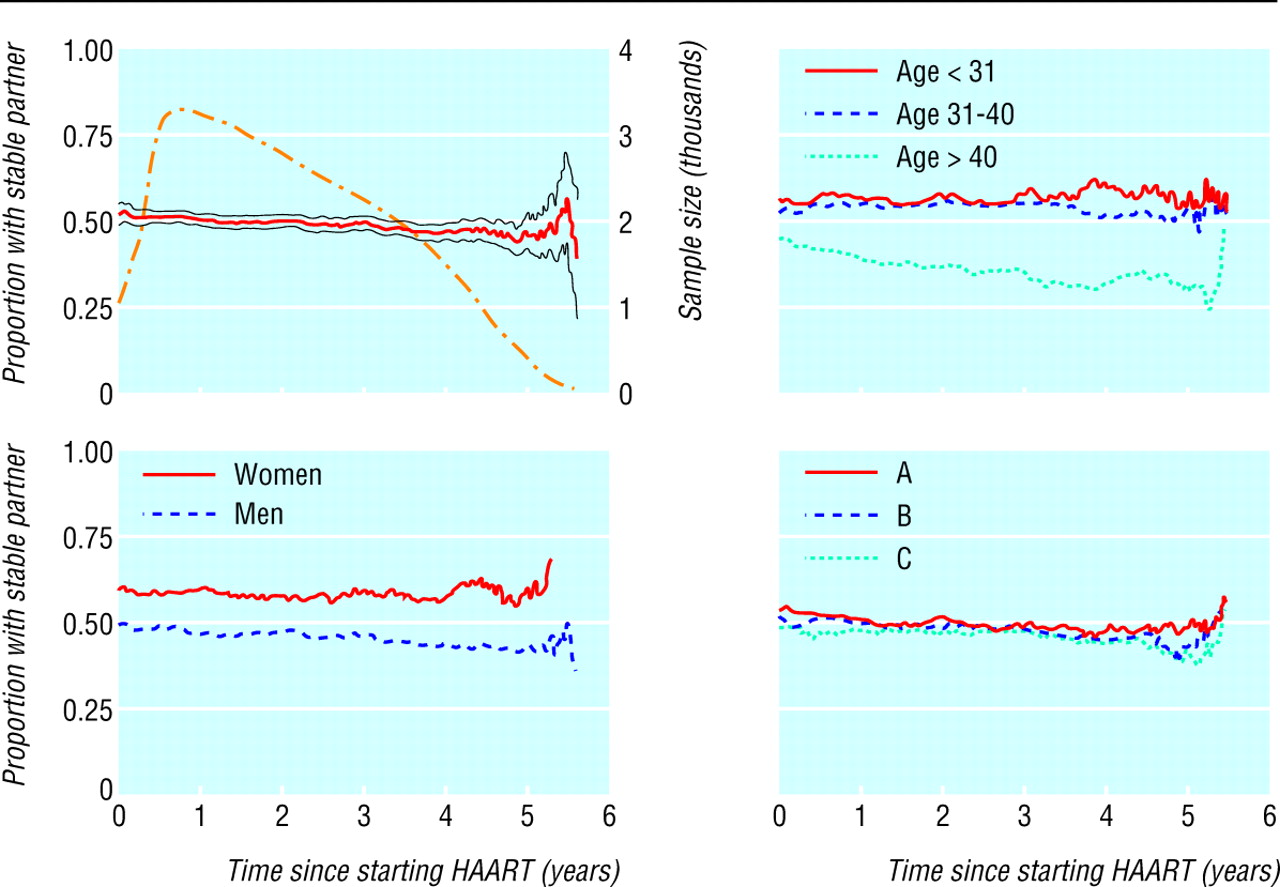
Proportion of participants reporting a stable partnership after starting highly active antiretroviral therapy (HAART): overall proportion (with 95% confidence interval) and sample size (dotted line) (top left); proportion for each sex (bottom left); proportion for each of three age groups (top right); and proportion for each clinical stage at baseline (bottom right)
{kind=link}
Of the 3736 patients in our analysis, 2985 (80%) reported a stable partnership at least once during follow up. Those who had had antiretroviral therapy before starting HAART were likely to have registered earlier with the cohort and therefore had more time in which to form stable partnerships (table 2). Among the participants who had had previous antiretroviral therapy, the percentage reporting a stable partnership at least once was slightly higher for those at clinical stage A (484/565, 86%) than for those at stage C (416/511, 81%). This may reflect a higher mortality among patients who were sicker when starting HAART.
Number (percentage) of participants in each stratum reporting stable partnership at least once
Of the 3432 (92%) participants who achieved optimal viral suppression (RNA < 400 copies/ml) at least once, 3360 (98%) had a CD4 cell count measured within the three months before they first achieved optimal suppression. We used these 3360 participants to estimate the association between stable partnership and the rate of progression to viral rebound.
Primary endpoint
Kaplan-Meier curves show that the initial rate of new disease or death was higher for patients starting HAART without previous antiretroviral therapy (fig 2). This is probably a result of immune restoration diseases (new disease within 90 days of starting HAART without previous antiretroviral therapy) rather than HIV progression.20 Log-log survival curves (not shown) for both baseline CDC group and previous antiretroviral therapy suggest that a proportional hazards assumption is not realistic for either variable.

Proportion of participants without new CDC group C disease or death over time after starting highly active antiretroviral therapy (HAART). Kaplan-Meier curves for each clinical stage (A, B, and C) at baseline for participants with previous antiretroviral therapy (top) and for those without previous antiretroviral therapy (bottom)
{kind=link}
Across strata formed by each combination of baseline CDC group and previous antiretroviral therapy, a stable partnership was associated with a slower rate of progression to new CDC group C disease or death (hazard ratio 0.79, 95% confidence interval 0.63 to 0.98) (table 3). Exclusion of probable immune restoration diseases did not alter the result (hazard ratio 0.77, 0.61 to 0.97). We found no evidence of an interaction between stable partnership and either baseline CDC group (difference in log likelihood ratio 0.9, df = 2, P = 0.64) or previous antiretroviral therapy (0.1, df = 1, P = 0.74). This suggests that stable partnership had a similar association with disease progression in each stratum. Nor did we find any evidence that a stable partnership had a different association if it first occurred after April 2000 (difference in log likelihood ratio < 0.1, df = 1, P = 0.94), and our estimate of this association did not change when we included in our definition those reporting a stable partner without sexual intercourse. This indicates that the change in the way questions were asked did not materially influence our estimates of the association between stable partnership and disease progression.
Cox proportional hazards model for time to new CDC group, stage C disease, or death
Estimates for covariates (table 3) show that the rate of progression to new CDC group C disease or death increased with increasing viral load at baseline, with increasing age, and among intravenous drug users but decreased with increasing CD4 count at baseline. We found no evidence that the association between disease progression and stable partnership was any different for intravenous drug users (difference in log likelihood ratio 0.49, df = 1, P = 0.48).
Of 3309 patients who did not experience new CDC group C disease or death, 2896 (88%) attended a follow up during the 12 months before 28 February 2002. We found no evidence of a “walking well” phenomenon, whereby patients with less severe disease were less likely to attend follow up. Compared with participants who had attended a recent follow up, those who had not were at a similar clinical stage at baseline, with similar baseline viral load and CD4 cell count (table 1).
Secondary endpoints
Stable partnership was associated with a decrease in the rate of progression to death and an increase in the rate of progression to CD4 cell counts of 50 and 100 above those recorded at baseline (table 4). We also found weaker evidence that stable partnership was associated with both an increase in the rate of progression to optimal viral suppression (hazard ratio 1.06, 0.98 to 1.14) and, in those achieving optimal suppression, with a decrease in the rate of progression to viral rebound (hazard ratio 0.91, 0.80 to 1.04).
Adjusted hazard ratios for the association between stable partnership and each endpoint
Discussion
Our analysis shows that a stable partnership is associated with a slower rate of disease progression in HIV infected patients receiving highly active antiretroviral therapy. The evidence for this is consistent across a range of surrogate marker and clinical endpoints. Our “intention to treat” definition of stable partnership was designed to avoid a liberal bias but may underestimate the strength of the association between stable partnership and disease progression. If, as figure 1d suggests, sicker patients are no more likely to discontinue stable partnerships because of the severity of their disease, then we could represent stable partnership as a variable that switches on and off as partnerships start and end. With this “as treated” definition, stable partnership is associated with a far greater decline in the rate of progression to new CDC group C disease or death (hazard ratio 0.67, 95% confidence interval 0.55 to 0.81).
Our analysis has several possible limitations. Firstly, exclusions and censoring could lead to bias. Bias through informative censoring is unlikely, because 88% of those censored had been seen in the previous year. However, we excluded 30% of participants in the Swiss HIV cohort study who were taking HAART from our analysis, mostly because of missing baseline data. Predicting the direction of any bias is difficult, but clearly bias is possible.
Secondly, although we adjusted for the severity of the disease at baseline, a patient's health changes over time. “Time dependent confounding” occurs if sicker patients are less likely to form stable partnerships and these people are sicker because they were unable to form stable partnerships in the past.21 The effect of stable partnership is then confounded with disease severity. Many other factors—for example, mental health, drug adherence, and treatment efficacy—are potentially confounded with stable partnership in this way. Establishing a causal relationship with observational data is difficult. We have shown that after adjustment for baseline covariates an association remains between disease progression and stable partnership. The absence of a stable partnership is therefore a marker for an increased rate of disease progression, but that does not mean that the absence causes the increase.
Thirdly, the presence or absence of a stable partnership is an important but incomplete measure of the many ways in which social relationships influence health. Our definition of a stable partnership is likely to reflect received emotional support. One study to examine various aspects of social support found that greater emotional support was associated with a lower mortality in elderly people but that greater tangible support and the presence of a partner were not.8 However, the presence of a partner may be more important for younger adults.1
We can only speculate about the reasons why a stable partnership is associated with a slower rate of disease progression for people with HIV. The increased rate of progression to a CD4 cell increase and to viral suppression in patients with stable partners may be linked to drug adherence.22 People with a stable partner may have less depression,23 24 a risk factor in many other chronic diseases. Research is needed on the mechanisms through which social support could influence HIV infection and should focus on mechanisms that are amenable to intervention. Increased support from healthcare givers might improve outcome in HIV infected people, but the evidence from one randomised trial in chronic cardiac patients does not support this hypothesis.25
Conclusion
The presence of a stable partnership is associated with a slower rate of disease progression in HIV infected patients who receive HAART, but the reasons for this are unknown. For a healthcare professional caring for someone with HIV, the absence of a stable partnership indicates that this patient may progress more rapidly through clinical latency to the later stages of the disease.
What is already known on this topic
Social support has been associated with lower mortality among elderly people and people with cardiovascular disease
For people with HIV infection, social support has been linked to a slower decline in CD4 cell count, better adherence to treatment, and reduced risk behaviour
Little is known about the effect of social relationships on outcome in HIV infection
What this study adds
A stable partnership is associated with a slower rate of progression to AIDS or death in patients with HIV receiving highly active antiretroviral therapy
In the absence of a stable partnership an HIV infected patient may progress more rapidly through clinical latency to the later stages of the disease
Swiss HIV Cohort Study Members: M Battegay, E Bernasconi, H C Bucher, P Bürgisser, M Egger, P Erb, W Fierz, M Fischer, M Flepp, P Francioli (president of the SHCS, Centre Hospitalier Universitaire Vaudois, CH-1011-Lausanne), H Furrer (chairman of the clinical and laboratory committee), M Gorgievski, H Günthard, P Grob, B Hirschel, L Kaiser, C Kind, T Klimkait, B Ledergerber, U Lauper, M Opravil, F Paccaud, G Pantaleo, L Perrin, J Piffaretti, M Rickenbach (head of data centre), C Rudin (chairman of mother and child substudy), J Schupbach, R Speck, A Telenti, A Trkola, P Vernazza (chairman of the scientific board), T Wagels, R Weber, S Yerly.
Footnotes
-
Contributors HCB, RS, SDG, and JY designed the study. JY did the statistical analysis. MR, PV, MF, HF, EB, MB, BH, AT, and RW were responsible for patient recruitment, clinical assessment, and development of the questionnaire. MR was responsible for data quality. HCB, SDG, RS, and JY wrote the final report, assisted by all coauthors. HCB is the guarantor.
-
Funding This study was financed in the framework of the Swiss HIV cohort study, supported by the Swiss National Science Foundation (Grant no 3345-062041). The Basel Institute for Clinical Epidemiology is supported by a grant from santésuisse and the Gottfried and Julia Bangerter-Rhyner-Foundation. HCB and JY received research grants from santésuisse and the Gottfried and Julia Bangerter-Rhyner-Foundation.
-
Competing interests None declared.
-
Ethical approval The Swiss HIV cohort study was approved by the local ethical committees of the participating centres.