Article Text

Abstract
The incidence of acute hepatitis B virus (HBV) infection is higher among South Asian than among non-South Asian UK residents, and infections in South Asians occur more often during childhood. The UK’s immunisation policy should be changed to protect ethnic minority children against HBV infection.
- hepatitis B virus
- HBV
- ethnic groups
- immunisation policy
- UK
Statistics from Altmetric.com
In the UK, hepatitis B virus (HBV) infection is more prevalent among minority ethnic groups than others, particularly in people born abroad.1 This has limited implications for UK control policy, as the prevalence of HBV infection in ethnic minorities reflects infection risks both prior to and since immigration. The main source of data on the incidence of HBV infection in England and Wales is the routine laboratory surveillance of acute hepatitis, but direct estimates of the incidence among minority ethnic groups resident in the UK are not available. Using a validated method based on names to assign South Asian ethnicity we have compared the epidemiology of acute HBV infection in South Asian and non-South Asian ethnic groups. In addition, we compared the incidence of new HBV infections in blood donors of South Asian and other ethnicity.
METHODS
Acute HBV infections and associated risk factors reported by laboratories in England and Wales between 1 January 1988 and 31 December 2000 were studied. Reported names are held temporarily on the laboratory surveillance database in agreement with guidance on confidential patient information (http://www.doh.gov.uk/ipu/confiden/index.htm). “Nam Pehchan” software2 was used to assign South Asian ethnicity based on names. As previously described,3 to calculate incidence of infection from laboratory reports, infections were assumed to be symptomatic in 10% of cases under 15 years of age and in 33% of cases of 15 years and older. It was assumed that 75% of all symptomatic infections were reported and, conservatively, all infections reported in cases aged ⩽2 years were regarded as perinatally acquired and so excluded from incidence and cumulative incidence estimates. (Perinatal transmission has been largely preventable in the UK since April 2000 by the introduction of universal antenatal screening and vaccination of infants at risk.) The number of new infections that became chronic was estimated by applying an age dependent risk of developing chronic infection4 for cases up to age 20, and a risk of 4% for older cases. Denominators were obtained from mid-1997 population estimates (Office for National Statistics).
The number of new HBV infections (acute infections and seroconversions) among blood donors in England and Wales tested between 1 October 1995 and 30 June 2000 were grouped by reported ethnicity. The proportion of South Asian and non-South Asian donors among all tested donors was estimated using “Nam Pehchan” software on a sample of 26 970 named donors, selected to be representative of UK blood donors.
RESULTS
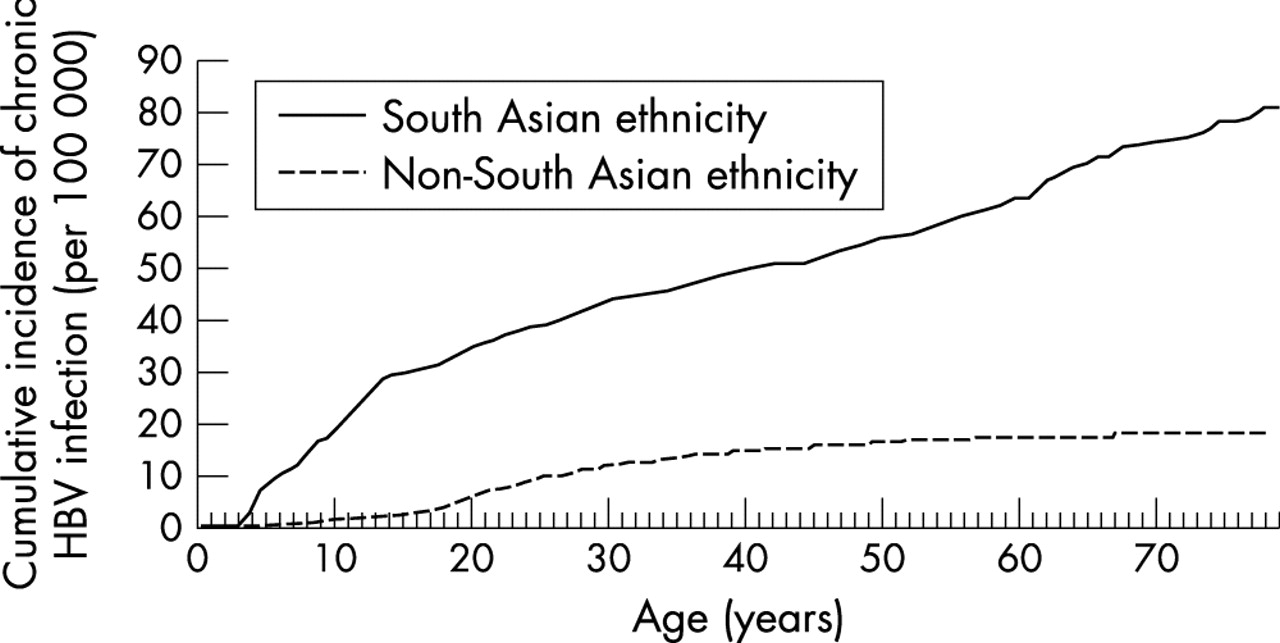
Between 1988 and 2000, an annual average of 635 cases of laboratory confirmed acute HBV infection was reported, of which 79% included names. Of named records, 8.5% (555) were identified as South Asian. The adjusted HBV incidence was 3.1 times higher in South Asians than in non-South Asians (14.9 and 4.8 per 100 000 person years, respectively; 95% confidence interval (CI) incidence ratio 2.8 to 3.4). The estimated lifetime risk of infection was 1.4% in South Asians and 0.4% in non-South Asians, and of chronic infection was 0.08% in South Asians and 0.02% in non-South Asians (fig 1).
{kind=link}
Estimated cumulative incidence of chronic HBV infection per 100 000 population by ethnicity, based on laboratory surveillance of acute HBV infection in England and Wales, 1988–2000, adjusted for asymptomatic infections and under-reporting and excluding infections in children ⩽2 years of age.
In South Asian blood donors the frequency of new HBV infections was 4.3 times higher than in non-South Asian blood donors (95% CI 1.1 to 11.8).
Nine per cent (51 cases) of reported acute HBV infections in South Asians were children (age <15 years), significantly higher than this proportion in non-South Asians (1.7%; 99 cases; p<0.0001). Of South Asian cases in children, 22% (11 cases) were 2 years of age or less, compared to 30% of non-South Asian cases in children (30 cases; p = 0.3). After excluding all cases ⩽2 years of age, the adjusted incidence of acute HBV infection was 10 times higher in South Asian children than in non-South Asian children (10.5 and 1.0 per 100 000 per year, respectively; 95% CI incidence ratio 6.9 to 15.4). The most frequent source of infection for South Asian children >2 years of age was within the household (11 cases; 61% of cases with a risk factor reported); 45% of infections (18 cases) in South Asian children >2 years of age were reported to have been acquired overseas.
DISCUSSION
Our study shows that South Asians are at higher risk of HBV infection than non-South Asians while resident in England and Wales, particularly in childhood. A high incidence of HBV infection has also been shown among UK born children of Somali ethnicity resident in the UK,5 suggesting that significant transmission during childhood may occur among UK ethnic minorities who originate in high or intermediate prevalence countries.
Preventing HBV infections in children needs special emphasis, as the risk of developing chronic infection is higher in children than adults.4 Chronic HBV infection sustains HBV transmission in the population and its sequelae constitute most of the associated burden of disease. For non-South Asians, HBV infection in childhood is rare. By contrast, we found that HBV infection among South Asian children in England and Wales is more common, with transmission within the household (and while travelling) frequently reported. Both are unlikely to be prevented by the current UK selective vaccination policy.
Our data suggest that infant immunisation targeted at UK resident ethnic minorities originating from HBV endemic areas could significantly reduce HBV transmission. Such a policy was recommended in 1990 in the United States,6 and started in the Netherlands in 2003 (http://www.gr.nl/adviezen.php?ID=730). In the USA, coverage achieved with this policy was limited, possibly due to difficulties targeting vaccination based on ethnicity.6
In the UK, universal infant HBV immunisation in geographical areas with a high proportion of ethnic minorities may be more acceptable and feasible than targeting individual families on the basis of ethnic status. Such a policy would be similar to the universal neonatal BCG immunisation programme currently used in some areas. To avoid additional visits or additional injections, the vaccine could be given in combination with other routine childhood immunisations, and has the potential to achieve high coverage in ethnic minority children at risk of hepatitis B.
Acknowledgments
We are grateful to all laboratories reporting acute HBV infections to the Public Health Laboratory Service Communicable Disease Surveillance Centre’s Immunisation Division, Usha Gungabissoon for help with the laboratory data, André Charlett for statistical advice, and the National Blood Service for providing data about blood donors.