Article Text

Abstract
Background and Aims: Following recent reports of increased numbers of adolescents being diagnosed with the adult or type 2 form of diabetes we aimed to describe the prevalence of both type 2 and other forms of diabetes in an urban population of children and young people in northern England.
Methods: A hospital based cross sectional study was performed in patients aged ≤30 years attending diabetic clinics in Leeds during the year 2000.
Results: A total of 677 subjects were identified, of whom 621 (92%) and 37 (5%) had type 1 and type 2 diabetes respectively. Four patients had confirmed maturity onset diabetes of the young, while the cause was uncertain for four. Median age of all patients was 22 years, with 396 (58%) aged 20–30; 32/37 patients with type 2 diabetes were aged 20–30. The prevalence of type 2 diabetes was 0.13 per 1000 overall, compared to 2.2 per 1000 for patients with type 1 diabetes. Of all type 2 diabetes patients, 24% were south Asian compared to 5% of the background population; 87% were categorised into the two least affluent tertiles of the Townsend score. This link with deprivation was not explained by the proportion of Asian patients across tertiles (approximately 25%).
Conclusions: This study shows extremely low prevalence of type 2 diabetes in 10–19 year olds, but will provide a baseline for future comparisons. Overall, type 2 diabetes is seen more commonly in south Asians, and an association with deprivation is suggested.
- type 2 diabetes mellitus
- prevalence
- young adults
Statistics from Altmetric.com
There is a clear need to assess the quality and provision of care for children and young people with diabetes, given that this is a condition that has long term complications and on which the UK National Health Service (NHS) currently spends almost 10% of its annual budget.1 The focus on young people is particularly crucial because of the clear evidence that improved diabetic control through the maintenance of blood sugar levels leads to fewer complications and lower morbidity and mortality.2–4
In order to maintain equity in the provision of care the planning of resource allocation needs to be based on reasonable estimates, not only of the number of individuals representing the overall burden of disease, but also quantifying the likely use of NHS services. At local level good information systems and diabetes registers can facilitate the provision of this type of information.5
Leeds is the second largest health authority in England with a densely urbanised population of 725 000 living in a compact geographical area of 560 km2. South Asians comprised 5% of the local population in the 1991 census. Diabetes services for those diagnosed aged 30 and under are based at four hospital sites which function as part of the Leeds Teaching Hospitals NHS Trust, one of the largest Trusts in England with a population of 300 000 aged 0–30 years.
In the light of reports suggesting an impending epidemic of adult or type 2 diabetes in our teenage population,6–9 we aim to determine the prevalence of all forms of diabetes, including type 2, in children and young adults attending the hospital clinics in a large UK city. Since the risk of type 2 diabetes is known to be higher in Asian adult populations,10,11 we wanted to determine whether or not this was the case for a younger population. Finally we wished to examine the influence of socioeconomic status on the prevalence of type 2 diabetes.
METHODS
Information was collected on all children and young people aged 30 years and under who attended a hospital diabetes clinic within the city of Leeds during the year 2000. Patients were identified using diabetes clinic lists for the paediatric, adolescent, and adult clinics from the following hospitals: the General Infirmary at Leeds (LGI), Wharfedale General Hospital, St James’s University Hospital (SJUH), and Seacroft Hospital. Within the health authority it is well established practice for all newly diagnosed children and young adults, irrespective of their type of diabetes, to be referred to a hospital clinic; the clinics have a policy of not discharging patients into primary care. The two major teaching hospitals (LGI and SJUH) have dedicated adolescent and young adult clinics to which patients in the study age group were referred. Data were collected by abstracting information from hospital records onto a customised form, designed by both paediatric and adult diabetologists, by a single experienced research assistant (CS). Items included both demographic details and clinical information, which were computerised using a customised database. The amount of clinical information that was systematically available for every patient was limited; partial recording in the notes of height and weight, for example, did not allow us to analyse body mass index or to investigate relations with obesity.
The diagnostic category of diabetes was determined from the hospital records and classified as type 1,12 type 2,13 maturity onset diabetes of the young (MODY), impaired glucose tolerance, and other forms of diabetes. Patients with other forms of diabetes included those categorised as “uncertain type 1 or type 2”, diabetes ascribed to a known cause (either secondary to pancreatectomy, haematoma, or lipodystrophy), insulin treated “J” type (West Indian) diabetes, and unclassified diabetes. This group was excluded from the analysis. Patients whose initial diagnosis was uncertain or MODY had their medical records examined by two clinicians (FC, HJB) who evaluated all the available information and reached a consensus diagnosis. Criteria for the diagnosis of MODY were (a) genetic testing and/or (b) clinical (that is, diagnosed under 25 years of age, five years off insulin treatment from diagnosis, and family history of a similar condition, usually with an autosomal dominant pattern).
A measure of deprivation, the Townsend score,14 was derived for each individual based on their address and validated postcode using information from the 1991 decennial census. This index of material deprivation is derived from the following four variables: unemployment, car ownership, housing tenure, and household overcrowding. Townsend scores for all postcodes in Leeds were ranked and then divided into tertiles. Identical cut offs were then used to divide the case data into tertiles, with a higher score representing a more deprived area. This areal based measure of socioeconomic status has been shown to be a fairly robust measure of an individual’s social class.15
A computer program16 was used to assign ethnic group to patients by identifying names of south Asian ethnic origin. This is based on full name and followed by visual inspection from an expert. The program has been shown to be accurate (90% sensitive, 99% specific) for the assignment of ethnic group to individuals in this way,17 and has been applied in other studies of ethnicity and paediatric chronic disease.18,19
Data were extracted from the customised database into Microsoft Access for further validation and checking, and then analysed using STATA.20 Prevalence was calculated for each age group using mid-year (2000) population estimates for the district of Leeds, which is co-terminus with Leeds Health Authority. Prevalence figures for south Asians and non-south Asians were derived using data from the 1991 Census. Exact 95% CI were calculated assuming prevalence followed a binomial distribution.
RESULTS
A total of 677 patients attending hospital clinics in Leeds during the year 2000 were identified. The majority (86%) were assigned to the care of six consultants at the two major Leeds hospitals (LGI and SJUH), two of whom were paediatricians. Of these patients, 231 individuals (40%) were designated as being under the care of a specialist paediatrician, with a median age of 12.5 years (quartiles 9.6, 15.9). Patients attending the smaller outlying clinics without specialist paediatric support were all over 15 years of age.
The majority of patients (396/677, 58%) were aged between 20–30 years with the median age of the whole group being 22.1 years (quartiles 15.5, 26.9). The median duration of diabetes was 7.0 years (quartiles 3.0, 12.5). The median age at diagnosis was 11.5 (quartiles 6.7, 17.2), with two thirds of patients diagnosed under 15 years.
Table 1 shows the numbers of clinic attendees according to their type of diabetes and the estimated prevalence of these conditions by age group. A total of 621/677 (92%) patients had type 1 diabetes and 37/677 (5%) had type 2 diabetes, while a further 19/677 (3%) had their type classified as “other”. This included uncertain type 1 or type 2 (n = 1), MODY (n = 4, aged 18–21), impaired glucose tolerance (n = 4), secondary diabetes (n = 6), insulin treated “J” type (West Indian) diabetes (n = 1), and other unclassified forms of diabetes (n = 3).
Comparative prevalence of diabetes (per 1000 population) in Leeds by age group
The prevalence of diabetes increased steadily with age, with a peak in 25–30 year olds of 4.4 and 0.5 per 1000 for type 1 and type 2 diabetes respectively. Overall prevalence was 2.2 and 0.13 for type 1 and type 2 diabetes. Prevalence of type 2 diabetes was significantly higher for south Asians than non-south Asians, both for 0–30 year olds combined (0.63 versus 0.10 per 1000; 95% CI 0.29 to 1.2 versus 0.067 to 0.15), and for 15–30 year olds (1.4 versus 0.17 per 1000; 95% CI 0.65 to 2.7 versus 0.11 to 0.25).
Thirty three (4.9%) of the 677 hospital attendees were south Asians (95% CI 3.4 to 6.8%), which was identical to the proportion of south Asians aged 0–30 years identified in the 1991 census. However, this proportion increased to 24.3% (95% CI 11.8 to 41.2%, n = 9/37) when we restricted the dataset to cases with type 2 diabetes (table 2). The proportion of patients with type 2 diabetes of south Asian origin was higher (40%) in the 10–19 year olds compared with the 20–30 year olds (22%), although there was no difference in the sex ratios by age. The median duration of disease for type 2 patients was typically two years, of which 5/37 of the patients with type 2 diabetes were diagnosed under the age of 15 years and 12/37 were diagnosed under 20. There was little variation in the proportion of Asians with age at onset, apart from the fact that no Asian patients were diagnosed between the ages of 20 and 24 years.
Distribution of cases of type II diabetes by age, sex, and ethnic group in Leeds
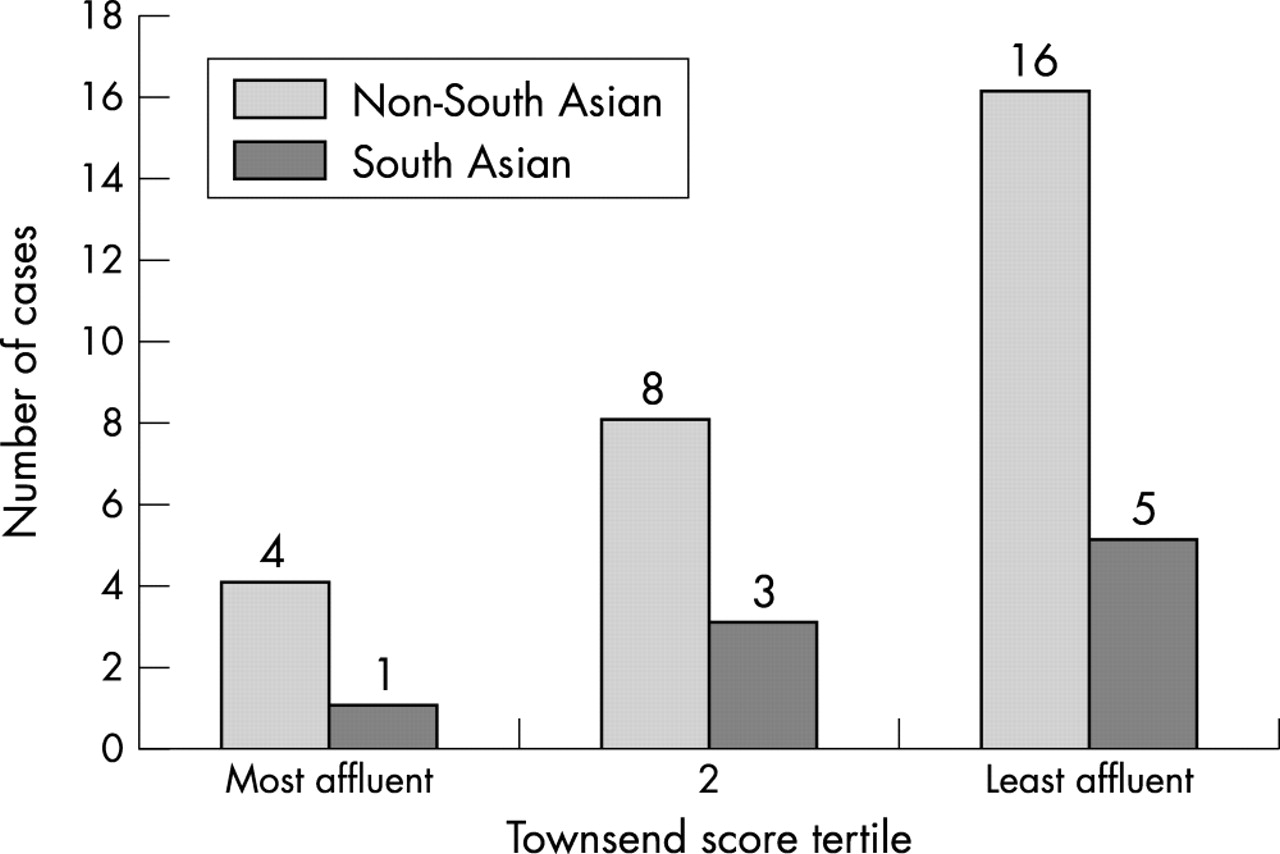
Figure 1 shows that the distribution of the Townsend score for the diabetic patients is similar to the socioeconomic profile of the population of Leeds (Mann-Whitney test, p = 0.73), with a median score of −0.4 (quartiles −0.4, 3.5) for all hospital attendees. However, the profile of patients with type 2 diabetes was generally less affluent, with a median score of 4.3 (quartiles −0.6, 6.9). Figure 2 also shows the socioeconomic profile of patients with type 2 diabetes by ethnic group. This shows the highest numbers of type 2 patients occur in the two least affluent groups, an effect which was independent of ethnic group (Mann-Whitney test, p = 0.99).
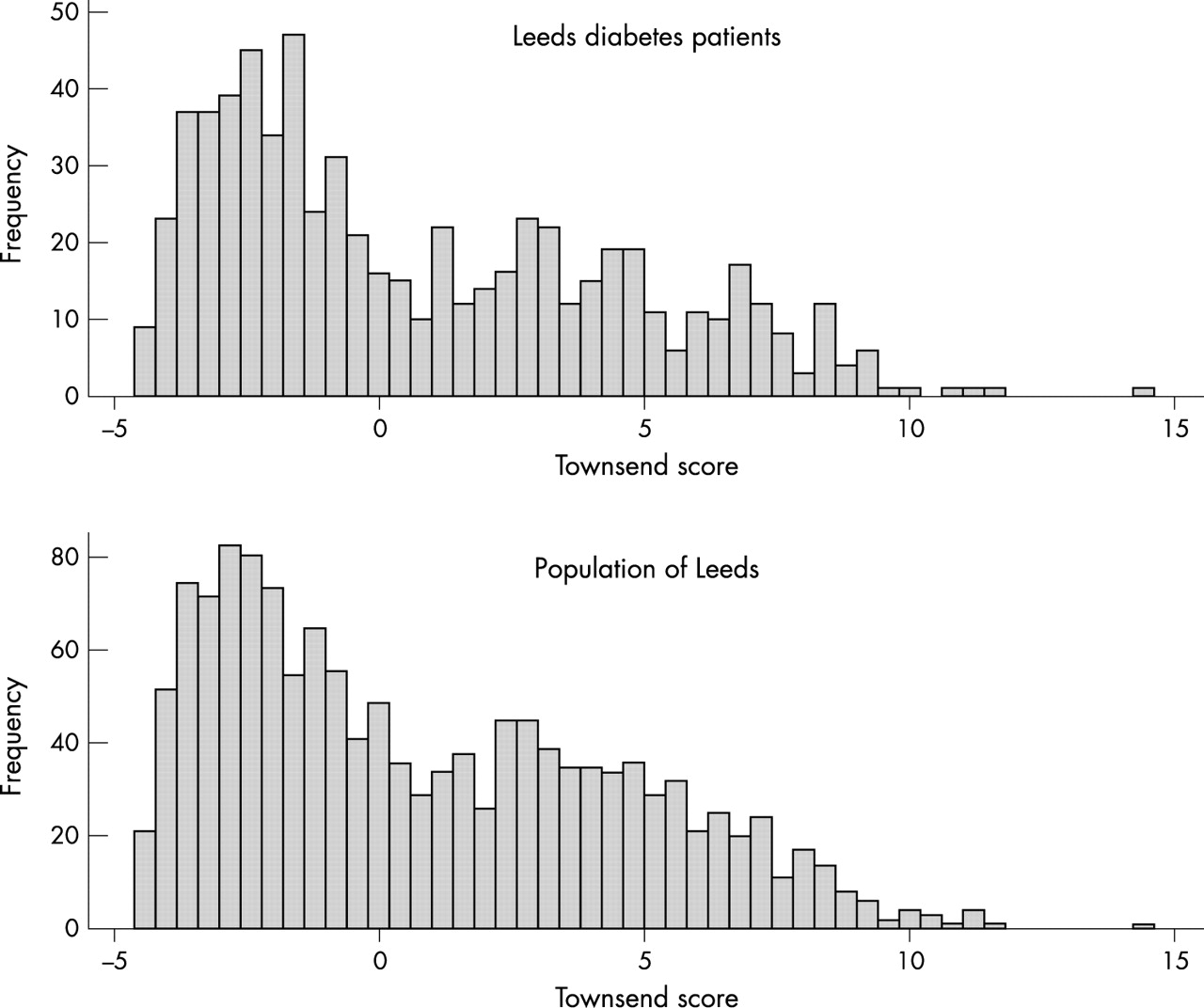
Comparison of the socioeconomic profile (Townsend score) of patients with diabetes and the population of Leeds.

{kind=link}
{kind=link}
Distribution of patients with type 2 diabetes across Townsend deprivation tertiles by ethnic group.
DISCUSSION
This study provides timely prevalence figures of diabetes occurring in young people aged 0–30 in the second largest metropolitan district in England. These data are an important requirement for health service planning. The novel findings for type 2 diabetes are presented in the context of a dearth of published baseline data in the UK, and are particularly important in light of suggestions of an impending epidemic in young people.7,21 Our data indicate that at present we are not facing a major public health problem with type 2 diabetes.
The prevalence of type 2 diabetes for young adults aged 15–30 in Leeds was estimated to be 0.23 per 1000 and 0.05 for those aged 10–19. In Birmingham, UK the estimated prevalence for under 18s was similar in 2000 at 0.038, showing this remains a rare chronic condition in this age range. Our data show clear differences in prevalence by ethnic group, with higher levels in south Asians aged 15–30 compared with non-south Asians (1.4 v 0.17, respectively) which taken together with the observations of Ehtisham and colleagues,22 show a consistent pattern of increased occurrence in young south Asians. This has clear implications for public health as we have now identified a high risk group who could be targeted for screening. Higher prevalence in other ethnic groups has been reported in the USA, ranging from 1 per 1000 in an American-Indian population23 to 50 per 1000 in Pima Indians aged 15–19 years.24
In considering whether our prevalence estimates represent the true burden of disease, a number of factors must be taken into account. A key issue is that diagnosis of type 2 diabetes is more likely to be misclassified, undiagnosed, or unreported than type 1.6 Our experience shows that clinicians treat diabetes empirically so that the aetiology is not always pursued. For example, few patients with type 2 diabetes had undergone testing for autoimmune antibodies in our study. Consequently, our classification of diabetes is based principally on clinical expert opinion, resulting in a few subjects for whom the diagnosis cannot be accurately defined. Despite this potential for misclassification, our results reflect what clinicians diagnose and treat and are therefore relevant to current healthcare in the city and can be extrapolated to other UK centres.
Another limitation is that our estimates may have excluded some eligible patients. This includes those who have never attended hospital, either because they were diagnosed and treated solely by general practitioners or they have failed to attend any appointments during the study period. In Leeds, the dominant patterns of referral from primary care are that virtually all paediatric patients are referred to hospital,25 and in the older age groups there is a well established tradition of referral to secondary care. Of 130 general practices in Leeds during 2000, only 47% reported having a clinic designed for adult diabetes patients. It is highly likely, particularly for teenagers, that they were referred to specialist hospital centres with experience of treating adolescents and young adults. Whilst accepting that we are more likely to have underestimated the numbers of older and therefore type 2 patients, we are confident that the figures are broadly representative, although possibly conservative.
A new observation is the association between type 2 diabetes and deprivation, with patients more likely to come from less affluent areas. If a relation existed between social class and obesity, this might explain the association between deprivation and type 2 diabetes, but there is little recent evidence to suggest a strong link between these two factors in children and young adults.26,27
Obesity and lack of exercise, known risk factors for type 2 diabetes, are both increasing in adolescents in western populations,28–30 and appear to be coincident with a rise in type 2 diabetes. Unfortunately we were unable to directly investigate these risk factors in our dataset. To facilitate future research on young adult patients, particularly where the diagnosis is unclear, efforts should be made within all treatment centres to collect current information on weight and height and ethnic background, in addition to regularly evaluating the classification and treatment.
Our findings fail to show an “epidemic” of type 2 diabetes in adolescents in Leeds, but monitoring of trends will continue. A higher prevalence of type 2 diabetes in south Asian teenagers and young adults is consistent with observations in adults. The increased risk of type 2 diabetes associated with less affluent socioeconomic groups is a new finding and will require confirmation in other populations. Future work will investigate this cohort in relation to diagnostic specificity and clinical outcomes, including diabetic control.
REFERENCES
Supplementary materials
. Acknowledgements
The following acknowledgements were unfortunately omitted from the article.We are grateful to Dr Jon Fear from Leeds Health Authority for providing financial support towards the collection and analysis of the data. Novo Nordisk are thanked for providing the Diabetes Patient Record System software. We also appreciate the help and assistance of all local clinicians (Dr P Holland, Dr P Sheridan, Dr MU Afza, Dr S Gilbey, Dr M Mansfield, Dr JK Wales, Professor PJ Grant) and their staff. Diabetes specialist nurses were especially supportive as were secretarial and medical records staff throughout the Trust. We also thank the Office for National Statistics for providing mid-year population estimates. Finally, we thank Roger Parslow for helpful comments on the manuscript.
Membership of the Leeds Diabetes Patient Record System Group (1999-2001)
Patricia McKinney, Carolyn Stephenson, Richard Feltbower (Paediatric Epidemiology Group), Trude Silman (former Community Health Council), Sue Jones, Sue Dodman (Clinical services managers), Linda Clapham, Virginia Nicholson (Diabetes Specialist Nurses), Fiona Campbell (Consultant paediatrician), H Jonathan Bodansky (Consultant Diabetologist), Deborah Quant (patient and IT consultant), Sally Casley, Gillian Richardson (Clinical Effectiveness), Joe Eastman (Health Economist), Judith Knapton (Primary Care), Debra Gill (IT systems)
Linked Articles
- Atoms
- Correction