Article Text

Abstract
Objectives: To estimate the compliance rates for the use of hip protectors among people living in residential care homes.
Population/setting: People aged 65 years and over living in residential care homes with 20 or more beds in East Kent, south east England.
Methods: Seventeen homes with the highest historical frequency of hip fractures were selected. All residents were offered SAFEHIP hip protectors. Care staff recorded daily hip protector compliance on diary cards over six months. Compliance rates were estimated from the number of sessions (morning, afternoon, evening, night) that a person wore hip protectors.
Results: A total of 153 (51%) out of 299 residents agreed to wear hip protectors The 24 hour compliance rate for those who were issued with hip protectors and wore them at least once was 29%: 37% in the daytime and 3% at night. Daytime compliance rates reduced from 47% for the first month, to around 30% for months 5 and 6.
Conclusion: This study highlights the problems of persuading older people living in residential care homes to wear hip protectors. They have been shown to prevent hip fracture in nursing home (high risk) populations, and a recent trial showed their effectiveness in a mixed geriatric population. People living in residential care homes are also at greater risk of falling and fracturing than their counterparts living in the community. Initiatives to prevent hip fracture within residential care homes are also justified.
- hip protectors
- compliance
- elderly
- fracture
Statistics from Altmetric.com
Falling among older people is a significant problem.1–5 Approximately 30% of people aged 65 and over living in the community fall each year, half of those do so repeatedly, and an estimated 50% of people aged 85 and over fall each year.1,6–10 The rate of falling among those living in institutions (excluding acute hospitals) has been estimated at 50%, with 10%–25% suffering severe consequences.11,12 One of the most serious consequences of falling is fractured neck of femur (hip fracture).8 The vast majority of fractured hips result from a fall.13 Around 1%–2% of community dwelling older people and 5%–7% of nursing home residents fracture their hip each year.8,14,15 The service cost of treatment and care of an older person with a hip fracture has been estimated at over £12 000 during the first year after hip fracture, at 1995/6 costs.3 Estimated one year mortality ranges from 12% to 25%, and fewer than half of surviving patients recover their pre-fracture levels of physical functioning.16–19
The principal ways of preventing hip fracture are: prevention of falls, ensuring bones are strong enough to withstand the impact after a fall, and/or protecting the hips with pads which deflect much of the energy away from the vulnerable area.20 This paper focuses on the latter of these interventions. Direct impact on and around the hip is the cause of the majority of hip fractures.1,3,21–25
Recent national guidelines, commissioned by the Department of Health in England, recommended that: “Hip protectors should be offered to all nursing home residents”.26 There have been a number of published trials that provide evidence for the effectiveness of hip protectors in preventing hip fracture in nursing home (high risk) populations,27–32 described in the review by Parker and colleagues.33 A further trial showed an estimated reduction in hip fractures of 60% in a mixed population of people living in geriatric long stay facilities and people living at home supported by health care centres.34
Hip protectors appear highly effective if the older person wears them; however, only a minority of older people appear to find them acceptable. Compliance rates in nursing homes, estimated using a variety of definitions and methods, of 44%–90% have been reported 28–32,35 Estimates of regular wearing of hip protectors in a nursing home has been as low as 24%27 and in “rest homes” as low as 30%.36 In a mixed geriatric population (long stay facility or home care) the compliance rate was 48%.34 Compliance rates are measured in consenting populations. The average rate can be far less if non-consenting older people are taken into account.
Like nursing home residents, people living in residential care homes are at substantially greater risk of falling than their counterparts living in the community. Consequently, initiatives that prevent hip fracture within residential care homes are also justified.
The aims of this work were to estimate compliance rates for the use of hip protectors among people living in residential care homes in East Kent Health Authority area of England (south east England, adjacent to the English Channel). The provision of hip protectors and the investigation of compliance were part of a larger study. Within this broad aim, the particular objectives were as follows:
-
To estimate the proportion of people who agreed in principle to wear hip protectors.
-
To estimate the 24 hour and daytime compliance rate.
-
To describe the variation in compliance over time and by residential care home.
Daytime compliance is of particular interest, since the majority of falls occur during the day.32 This is consistent with Kannus and colleagues who presented compliance as percentage of waking hours during which the hip protectors were worn,34 and with Villar and colleagues who monitored compliance through randomly timed visits.36
METHODS
Population
The target population for this work were people aged 65 years and over living in residential care homes with 20 or more beds in the East Kent Health Authority area.
Residential care homes provide accommodation, food, and personal care for different groups of people, including older people. They are staffed by a manager and care staff who, generally, are not professionally qualified. Homes are registered and inspected by county council social services departments. Nursing care is provided in the care home, if necessary, by community nurses. However, older people who are more frail and dependent upon nursing care are cared for in nursing homes.
East Kent is a health authority area in the south east of England and included an estimated 615 000 population (all ages) in mid-2000. It comprises 722 square miles (187 000 hectares), and contains five entire local authorities, and part of one other. It includes a spread of affluence/deprivation, with one local authority in the bottom 25% of deprivation, with the others lying within the interquartile range for the country. It includes two major inland towns, Ashford and the cathedral city of Canterbury, and the coastal towns of Margate, Ramsgate, Deal, Dover, and Folkestone. By far the greatest area of East Kent is, however, farmland. Table 1 gives a summary of the health authorities demographic make-up at mid-2000.
Demographic composition of East Kent relative to England, mid-2000
Selecting the sample of homes
The social services inspectorate supplied a list of every residential care home in East Kent. The list was used to identify homes that had provision for 20 or more beds. Homes that were duel registered (for residential and nursing home clients), or were offering specific care for learning disability or mental health difficulties, were excluded. The list of eligible homes was organised within primary care groups (PCG)*, and three homes within each PCG were selected sequentially from the list that had the highest frequency of fractured neck of femur over the previous five years. A further two homes were selected within one PCG, who had additional staff available to support the project. These had the next highest frequency of fracture neck of femur within the PCG.
The intervention
Every resident within the 17 homes was offered a fall risk assessment, with referral as necessary, reassessment, medication review, and three pairs of SAFEHIP hip protectors. (SAHVATEX A/S) The process included:
-
Contact with all staff involved.
-
Consent from general practitioners and home owners/managers for the study procedures.
-
Consent from the residents who took part.
-
Meetings with all primary care and residential care staff in the study areas.
-
Teaching of care staff in homes about falls risk and assessment.
-
Visits to homes to talk to residents about the project.
-
Offers of hip protectors to residents who consented.
-
An assessment to identify modifiable risk factors with referral to other services as appropriate.
-
Medication review and modification by pharmacists in conjunction with the general practitioner.
These are described in more detail below.
Individual letters describing the aims of the study and the proposed methods were sent to the social services inspectorate, general practitioners and other primary care staff, as well as residential home owners/managers. Written consent was obtained from general practitioners in order that assessment, appropriate referrals for problems identified, reassessment, and medication reviews could be undertaken by the project nurses and pharmacists. Consent was obtained from home owners/managers to ensure their cooperation in working with their staff and their residents. A patient information sheet explained every aspect of the project to the residents, and consent was obtained from residents taking part in the study.
Primary care and residential care home staff were each invited to attend a meeting within the PCG area. During the meetings, presentations were given regarding fall and fracture risk, the importance of medication review and the findings from previous research on hip protectors and compliance.
Within each residential home, project nurses carried out a two hour teaching session for care staff on fall and fracture risk and the importance of fall risk assessment. A teaching resource pack was collated and left with the staff. Before the assessment process began, project nurses visited each residential home and spent time in the communal sitting rooms in order to talk with residents. Hip protectors were left in each sitting room in order for residents and their relatives to familiarise themselves with them and to ask any questions.
All residents were offered SAFEHIP hip protectors. The protector is made of an outer shield of polypropylene with an inner plastozote lining and is sewn into special underwear so that it fits snugly over the greater trochanter. Three hip protectors were provided to residents who accepted the offer. This made it possible for one hip protector to be always available for wearing—that is, one for the wash, one to wear, and one available for the next day. Residents were given reassurance that they could change their mind regarding involvement in the study, that they could stop their involvement at any time, and that they could wear the hip protectors as much or as little as they chose. It was explained that a nurse would come to the home each week and assess how they were getting on.
Feedback to residential home owners/managers
Over the project period, residential home owners/managers and care staff received three letters. This informed them of the progress of the project and reminded them of the aims of the project, including the interest shown by local health and social service professionals who work with older people.
Falls risk factor assessment
Every resident was offered a single standardised assessment on entry to the study, to identify modifiable falls risk factors, by one of the project nurses. Two hundred and ninety nine out of 310 residents agreed to the assessment, which included questions on long term medical problems, postural hypotension, dizziness, walking/gait/balance/ability to transfer, vision problems, as well as falls history. If a falls risk was identified, referrals to appropriate professionals to modify these risk factors were made by residential home managers in conjunction with the relevant general practitioner. Clinical pharmacists visited each residential home and reviewed the medication for each resident. Changes recommended by the pharmacist that were agreed by the relevant general practitioner were implemented.
As well as an assessment to identify modifiable falls risk factors, project nurses collected relevant demographic information. Additionally, at the start of the study consenting residents were invited to complete a “fear of falling” questionnaire.37 Each consenting resident was reassessed in the care home by a project nurse after three months using an abridged version of the baseline assessment, to monitor change in risk factor status.
Compliance assessment
Project nurses encouraged specific care staff to take responsibility for the collection of compliance data. Each day was divided into four equal six hour sessions: morning (6:00–12:00), afternoon (12:00–18:00), evening (18:00–24:00), and night (24:00–6:00). Care staff recorded on a standardised A4 collection form whether hip protectors were worn during each session during each day of follow up. One A4 sheet captured compliance information for one patient over the period of one week.
The first assessments of residents took place in March 1999 and follow up ceased in December 1999.
Statistical analysis
The 24 hour compliance rate was estimated by counting the number of sessions that a person wore hip protectors divided by the number of sessions the protectors were available to wear (that is, from when the hip protectors were issued to the end of the study period or the end of follow up, whichever was sooner). Account was taken of the varying lengths of follow up due to death, hospitalisation or loss to follow up for other reasons in the calculation of the compliance rates. The daytime compliance rate was estimated in the same way but was restricted to morning, afternoon, and evening sessions only. Daytime compliance rates were also estimated for each of the first six months of the study, the period when the majority of the older people admitted to the study were followed up.
RESULTS
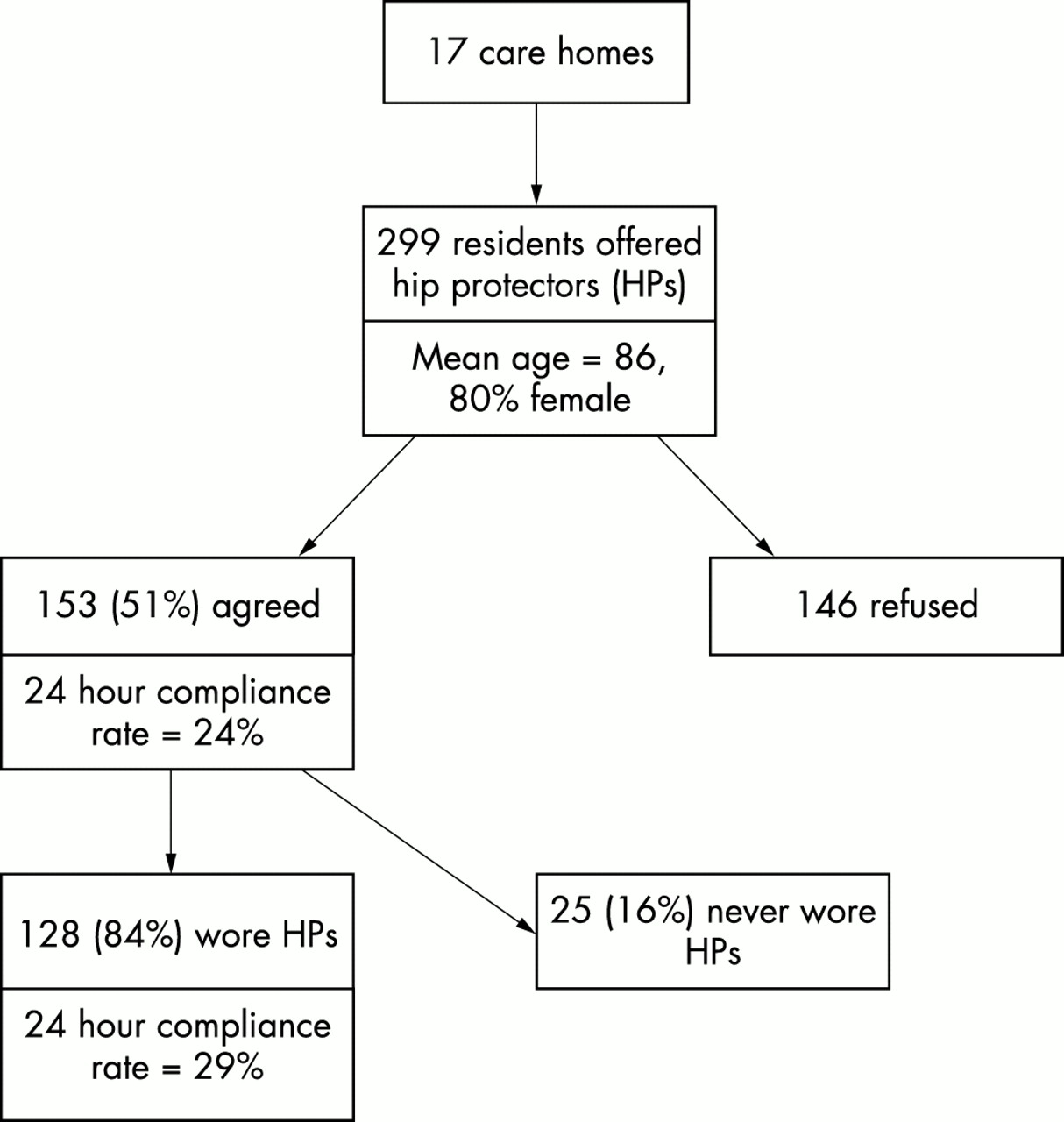
Seventeen homes were included in the study. The number of residents in each home varied from seven to 31. There were a total of 299 people living in the residential care homes who were invited to wear hip protectors. The characteristics of these residents are shown in table 2. Of these, 153 (51%) agreed to wear them and were issued with hip protectors (fig 1). This varied from 24% to 94% across the homes.
Characteristics of the care home residents as recorded at the baseline assessment

Residents included in the study with their 24 hour compliance rates.
The 24 hour compliance rate for residents who were issued hip protectors was 24%. Among the 153 people who were issued with hip protectors, 25 (16%) people reported never wearing them. In one home, none of the six residents who were issued with hip protectors wore them, and in another home only one out of eight people ever wore them. For the remaining results, the compliance rate is based on those who were issued with hip protectors and who ever wore them.
The 24 hour compliance rate for those who were issued with hip protectors and wore them at least once was 29% (fig 1). The compliance rates by time of day are shown in fig 2. The daytime compliance rate was 37%. The range of daytime compliance rates across homes was 0%–80%, with a median of 34%, and an interquartile range of 24%–40% (fig 3).

Hip protector compliance rate within residential care homes by time of day among those who were issued with and wore hip protectors.

Histogram of daytime compliance rates within residential care homes among those who were issued with and wore hip protectors.
Daytime compliance rates were examined by month and it was found that for the first month of wearing, compliance was 47%. Rates over 40% were obtained for the first three months and these declined to around 30% for months 5 and 6 (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trends in daytime compliance over the first six months of the study within residential care homes among those who were issued with and wore hip protectors.
DISCUSSION
Only 51% of people living in residential care homes indicated that they would wear hip protectors if issued, and of those, 16% did not wear them at any time. The 24 hour recorded compliance rate for those who were issued with hip protectors and who wore them at least once was 29%. This varied from 38% in the morning to 3% at night. Some have recommended wearing hip protectors 24 hours a day if the person is getting up two times or more during the night.38 One study found, however, that the majority of falls occur during the day.32
The compliance rate could be relatively low due to a failure of care staff to record that hip protectors were being worn. The average daytime recorded compliance rate was 37%, which is similar to a previous published report for residents of rest homes.36 This previous work used an alternative method of measuring compliance, namely through observation at randomly timed visits to the rest homes once a fortnight.
Hip protectors are a very important means of protecting older people from hip fracture, and are particularly beneficial to those who are at high risk of falling or who have brittle bones (osteoporosis). It has been shown that if an older person wears a hip protector, their annual risk of hip fracture is minimal. In five randomised controlled trials involving 1742 persons in nursing homes, only one person had a hip fracture while using hip protectors.39 Additionally, Kannus and colleagues reported that four hip fractures occurred while hip protectors were worn in their mixed geriatric population.34 All studies, including our own, have found that many older people are unwilling to wear hip protectors. For those who indicate they are willing to try them, a number change their minds when confronted by the hip protector, some forget to wear them, and some give up due to problems of fitting and discomfort.36 Increasing and maintaining compliance, therefore, is an important goal.
Key points
-
Hip protectors are a very important means of protecting older people from hip fracture, and are particularly beneficial to those who are at high risk of falling or who have brittle bones (osteoporosis).
-
Only 15% of people living in residential care homes indicated that they would wear hip protectors if issued, and of those, 16% did not wear them at any time.
-
The 24 compliance rate for those who were issued with hip protectors and those who wore them was 29%.
-
The daytime compliance rate was 37%.
-
For the first month of wearing, compliance was 47%, rates over 40% were obtained for the first three months, and these declined to around 30% for months 5 and 6.
-
Daytime compliance rate varied across residential care homes fron 0% to 80%. It is hypothesisied that carers who promote the use of hip protectors achieve high compliance.
When asked, people indicate the following concerns about hip protectors: appearance, comfort, fit, efficacy, ease of laundering, and cost.40,41 Cameron and Quine reported that probably the most crucial factors for compliance are concerns about the comfort of the hip protector, perception of personal risk of fall and fracture, and a belief by the older person that the fracture is preventable. Promotion to make older people aware of the prevalence, and the causes and consequences of hip fracture might motivate the older person to wear hip protectors despite the extra effort required and the discomfort caused by the protector.40 Even if the older person agrees to wear hip protectors, there may be difficulties for people who suffer incontinence, as well for people with weakness in their upper limbs who have difficulty pulling the garment down for toileting.42
Daytime compliance rate varied across residential care homes from 0% to 80%. The impression that we obtained during contact with the homes was that support for the promotion of hip protectors by the staff of the homes varied substantially, and that the best rates were obtained where the staff actively supported their use. This finding suggests a potentially fruitful avenue for investigation. It is hypothesised that carers who promote the use of hip protectors achieve high compliance. Conversely, it is hypothesised that older people living with carers who do not promote, or are negative towards, the wearing of hip protectors have much lower compliance rates. These hypotheses are supported by work by Ross and colleagues who gave evidence of increased compliance in the use of hip protectors if additional support is given when starting to wear the hip protector.43 Parkkari and colleagues believe that the attitude of the staff in the institutions was a crucial factor for reaching good compliance in their study.35 These hypotheses should be investigated further, and if they are found to be true, then a major focus of hip fracture prevention through the use of hip protectors should be the vigorous promotion to the carers of vulnerable older people.
CANTERBURY HIP PROTECTOR PROJECT TEAM
Other members of the Canterbury Hip Protector Project Team are: Charlie Manicom (Health Improvement Manager), Lesley Sinnock (Commissioner, Medical and Older People’s Services), Linda Dodds (Pharmaceuticial Advisor), Nick Morley-Smith (Specialist Registrar in Public Health Medicine), East Kent Health Authority; Ian Sturgess (Consultant Geriatrician), Neil Taylor, Salwa Morcos, Ann Tickner, Bridget Baxter, Carol Walker (Pharmacists), East Kent Hospital Trust; Kath Gill (Community Pharmacist), Gill Lewis (Service and Strategy Manager), Mary Sinclair, Teresa Wells, Gill Norford, Pauline Hammond, Lynn Turner, Liz Watson (Project Nurses), East Kent Community Trust.
Acknowledgments
Our thanks to the NHSE South East Regional Office R&D Directorate, and East Kent Health Authority who funded this project. Our thanks also to the staff and residents of the care homes included in this study.
REFERENCES
Footnotes
↵* Primary care in England was organised, during the study period, around primary care groups (PCGs) of general practitioners. East Kent included around 600 000 residents and was served by five PCGs, ranging in size from 100 000 to 160 000 patients.
-
↵* Other members of the Canterbury Hip Protector Project Team are listed at the end of the paper.