Article Text

Abstract
Background We examine the association between the poverty histories of neighbourhoods and three indicators of psychosocial well-being—depressive symptoms, sense of control and number of stressors—in an observational study of mothers of young children in California. We also consider if length of residence in a neighbourhood moderates the association between neighbourhood poverty history and psychosocial well-being.
Methods Data come from the Geographic Research on Well-being (GROW) Study, a subsample of mothers who completed the population-based California Maternal and Infant Health Assessment in 2003–2007 and were reinterviewed in 2012–2013. Poverty histories of neighbourhoods were constructed using the Neighbourhood Change Database (1970–2000) and American Community Survey (2005–2009). The analytic sample included 2726 women from GROW residing in 1906 census tracts.
Results Adjusting for individual socioeconomic and demographic characteristics, women living in neighbourhoods where poverty decreased over the 40-year period had lower odds of depressive symptoms and a greater sense of control than women living in long-term, low-poverty neighbourhoods. Women living in long-term high-poverty neighbourhoods or in neighbourhoods where poverty increased over the 40-year period reported lower sense of control than women living in long-term, low-poverty neighbourhoods and these effects were modified by length of time living in the neighbourhood. No significant effects of neighbourhood poverty histories were found for number of stressors.
Conclusions Policies aimed at reducing neighbourhood poverty may improve mothers' psychosocial well-being.
- Neighborhood/place
- POVERTY
- PSYCHOSOCIAL FACTORS
- STRESS
- DEPRESSION
Statistics from Altmetric.com
Introduction
Neighbourhoods play an important role in health and well-being.1 ,2 Residents of poor neighbourhoods are more likely to report worse mental health and greater psychosocial stress compared with residents of non-poor neighbourhoods, even after adjustment for individual-level socioeconomic characteristics.3–5 To date, most studies have measured neighbourhood conditions at one point in time even though neighbourhood conditions change due to economic, social and political circumstances.6 The purpose of our study is to examine the relationship between the poverty histories of neighbourhoods over a 40-year period and the psychosocial well-being of California mothers in 2012–2013.
The focus on the poverty history of a neighbourhood is significant because neighbourhoods are not static.7 Some presently poor neighbourhoods may have experienced years of concentrated poverty, racial segregation and disinvestments, resulting in lower quality schools and/or higher crime, whereas other presently poor neighbourhoods may have only recently experienced economic decline. Residents' current experiences within their neighbourhoods are likely shaped by these different histories.8 ,9 Residing in neighbourhoods with deteriorating conditions may be stressful and worrisome for its residents; for example, residents living in neighbourhoods with a higher concentration of deterioration report greater stress and depressive symptoms than residents living in neighbourhoods with a lower concentration of deterioration.10 Conversely, residing in neighbourhoods that have seen economic investment and declining poverty may be associated with more positive psychosocial well-being as long-standing issues of crime, public disinvestment and access to health-related resources improve. For long-term residents of these neighbourhoods, however, rising rents/property values and the influx of new residents may lead to displacement or change the dynamic of a neighbourhood, creating anxiety and stress in either case.11
Few studies have empirically examined the relationship between the economic history of a neighbourhood and residents' health. Among those that have, neighbourhoods experiencing long-term disadvantage or deterioration appear to exert the strongest negative health effects compared with long-term advantaged or stable neighbourhoods. In a nationally representative sample, mid-life and older adults residing in neighbourhoods that experienced increasing unemployment in the decade prior to the assessment of residents' health had higher levels of depressive symptoms compared with those living in neighbourhoods with stable unemployment, after adjusting for individuals' socio-demographic characteristics.12 In another study, stable, high-poverty neighbourhoods were associated with poorer cardiovascular outcomes compared with stable, low-poverty neighbourhoods among mid-life and older adult women.13 Finally, California women living in either long-term, high-poverty neighbourhoods or neighbourhoods experiencing increasing poverty had higher odds of preterm birth compared with women living in long-term low-poverty neighbourhoods, net of individual characteristics.14
The long-term poverty conditions of a neighbourhood may be important for psychosocial well-being and one's duration of residence in that neighbourhood may also play a role.5 ,15–22 Greater familiarity with one's neighbourhood may promote a heightened sense of control and lower feelings of anxiety and stress; alternatively, prolonged exposure to a chronically poor neighbourhood may lower feelings of control and increase anxiety and stress.8–10 For this reason, it is important to examine if residents' duration of residence modifies the effect of neighbourhoods' poverty histories on psychosocial well-being.
Our study investigates two main research questions. First, which neighbourhood poverty histories are associated with psychosocial well-being, as measured by depressive symptoms, sense of control and number of stressors? We explore these three outcomes because they capture different aspects of psychosocial well-being, including functioning (ie, depressive symptoms), resiliency (ie, sense of control) and stress (ie, number of stressors), and as such provide a more complete understanding of how the poverty histories of neighbourhoods shape residents' lives. We hypothesise that women residing in neighbourhoods characterised by long-term high poverty or increasing poverty will be more likely to report depressive symptoms and will report a lower sense of control and more stressors compared with women residing in neighbourhoods characterised by long-term low poverty. Second, does duration of residence strengthen these associations? We hypothesise that longer residence in a neighbourhood will be associated with better psychosocial well-being,9 ,16 but this association will be weaker among women who reside in neighbourhoods characterised by long-term high poverty than among women living in neighbourhoods characterised by decreasing poverty or long-term low poverty.
Data and methods
Data
Data come from the Geographic Research on Well-being (GROW) Study, a subsample of women who completed the California Maternal and Infant Health Assessment (MIHA) in 2003–2007 and were reinterviewed in 2012–2013.23 The MIHA study, from which GROW is drawn, is an annual, cross-sectional, statewide representative survey of postpartum women who delivered live infants in California from February to May since 1999. Women were eligible for MIHA if they spoke English or Spanish, were residents of California, were aged 15 or older, delivered singleton, twin or triplet births, and provided their addresses on the birth certificate.
The GROW sample consists of 3016 women who were living in six largely urbanised California counties when they completed the MIHA survey: Alameda, Los Angeles, Orange, Sacramento, San Diego and Santa Clara. The response rate for MIHA 2003–2007 was at least 70% each year. The response rate for GROW was 33% of the eligible sample and 75% of located women.23
We use census tracts as approximations of neighbourhoods, following prior research.24 ,25 Census-tract poverty rates (ie, percentage of residents below the federal poverty level (FPL), a threshold set by the US government annually and calculated based on families' income, size and composition)26 were used to construct the poverty histories of neighbourhoods (see figure 1). The Neighborhood Change Database (NCDB) provided poverty data from 1970 through 2000 and the American Community Survey (ACS) provided data for the final time period (2005–2009). Data in the NCDB are from the decennial censuses collected by the US Census Bureau. The ACS is an annual survey also conducted by the US Census Bureau that collects similar data to the decennial census. Geographic tract boundaries change over time; therefore, in the NCDB and ACS, data have been recalculated and weighted to correspond to 2000 Census boundaries so that the tract data are comparable over time.
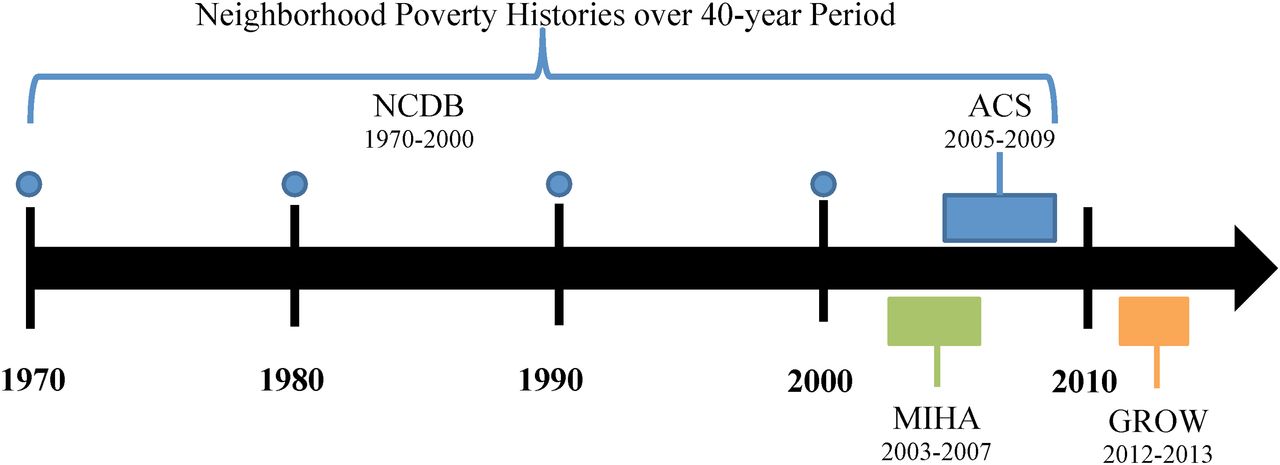
Summary of neighbourhood data and survey data collected for study. ACS, American Community Survey; GROW, Geographic Research on Well-being Study; MIHA, Maternal and Infant Health Assessment.
Neighbourhood data were linked to the GROW data set. On average, 1.4 GROW respondents resided in each tract (range 1–9); 90% of tracts included only one or two GROW respondents. For the current analysis, we included women who were living in California at the time of the GROW survey, whose addresses geocoded accurately to a census tract, and who reported their race/ethnicity on MIHA as Asian/Pacific Islander, black, Latina or white. Our final sample consists of 2726 women residing in 1906 census tracts.
Measures
Outcomes. We examined three indicators of psychosocial well-being—depressive symptoms, sense of control and number of stressors—assessed in 2012–2013; 5–10 years post partum.
Depressive symptoms were assessed by asking women to report whether they had experienced feelings of sadness, emptiness or depression for 2 weeks or more over the past 12 months (yes/no).
Sense of control. The Pearlin Mastery Scale measures individuals' sense that forces in their life are under their control.27 Respondents were asked how strongly they agreed with the following 7 items (1= strongly agree, 4= strongly disagree): there is no way I can solve some problems I have; I feel I am being pushed around in life; I have little control over things that happen to me; I can do anything I set my mind to; I often feel helpless in dealing with problems; what happens in the future depends on me and there is little I can do to change important things. Negatively worded items were reverse coded such that higher values indicate higher sense of control (α=0.80).
Number of stressors is a tally of affirmative responses to nine stressful life events experienced within the past 12 months: had to move because couldn't pay rent/mortgage, did not have a regular place to sleep, was homeless, partner lost job, respondent lost job, employment hours or pay were cut (self/partner), went to jail (self/partner), someone close to respondent had a drinking/drug problem and respondent experienced intimate partner violence.
Measures of neighbourhood poverty histories. We used census tract poverty rates from NCDB and ACS data and categorised neighbourhood-level poverty as low (<5%), moderate (5–20%) and high (>20%) at each of the five time periods (1970, 1980, 1990, 2000 and 2005–2009). The threshold for high poverty (≥20%) was selected using the US Census Bureau's definition of poverty areas.28 No established thresholds for low and moderate poverty neighbourhoods exist, so we selected <5% as our threshold for low poverty under the assumption that this represents a neighbourhood with few poor families. We then categorised neighbourhoods into five poverty histories: (1) long-term low poverty (low poverty or a combination of low and moderate poverty in all time periods without any discernable pattern); (2) long-term moderate poverty (moderate poverty in all time periods); (3) long-term high poverty (high poverty or a combination of moderate and high poverty in all time periods with no discernable pattern); (4) increasing poverty (low to moderate poverty, low to high poverty or moderate to high poverty between the first and last period) and (5) decreasing poverty (moderate to low poverty, high to moderate poverty or high to low poverty between the first and last period). Long-term low-poverty neighbourhoods serve as our referent group because these represent the most economically advantaged neighbourhoods. For further details, see Margerison-Zilko et al.14
Covariates. We included covariates: (1) we hypothesised may influence selection into neighbourhoods and (2) are associated with psychosocial well-being: maternal age (in years), self-reported race/ethnicity (Asian or Pacific Islander, non-Hispanic black, foreign-born Latina, US-born Latina and non-Hispanic white), relationship status (married or cohabitating vs not married and not cohabitating) and number of children in household. Two indicators captured individuals' socioeconomic status (SES)—educational attainment (less than high school, high school graduate or General Education Development degree (GED), some college and college graduate) and income to poverty ratio (<100% FPL, 101–200% FPL, 201–400% FPL and >400% FPL). Missing income values were imputed using hot-deck methodology and the following variables: maternal age, race/ethnicity, education, employment, marital status and neighbourhood poverty. Finally, women reported the duration of residence in their current neighbourhood, which we used as a continuous variable, ranging from <1 month to >10 years.
Except for race/ethnicity, all measures are from GROW.
Statistical analysis
First, we examined the per cent of women residing in each of the neighbourhood types. Next, we examined the prevalence and level of psychosocial well-being as well as other characteristics of women across neighbourhood types. We used logistic regression (depressive symptoms), linear regression (sense of control) and zero-inflated Poisson (number of stressors) to investigate the association between neighbourhood poverty histories and three indicators of psychosocial well-being. For each outcome, we estimated three models. Model 1 estimates the association between neighbourhood poverty histories and psychosocial well-being, net of demographic covariates. Model 2 further adjusts for women's SES. Model 3 tests whether associations between neighbourhood poverty histories and psychosocial well-being depend on duration of residence in the neighbourhood by including a set of interactions between duration of residence and neighbourhood type. All analyses apply survey weights to account for the complex sampling design of GROW and were conducted using SAS 9.2.
Results
Almost three-quarters of women lived in long-term low-poverty (24.2%), long-term moderate-poverty (22.7%) or increasing poverty neighbourhoods (24.3%). Approximately 19% lived in long-term high-poverty neighbourhoods, whereas 9.4% of women lived in decreasing poverty neighbourhoods.
Table 1 shows that 17–23% of women reported depressive symptoms across neighbourhood types, with the exception of women residing in decreasing poverty neighbourhoods who reported significantly lower rates of depressive symptoms (9.8%). Women residing in long-term low-poverty and decreasing poverty neighbourhoods reported higher sense of control than long-term moderate-poverty, long-term high-poverty and increasing poverty neighbourhoods. Similar patterns were found for number of stressors, with women residing in long-term low-poverty and decreasing poverty neighbourhoods reporting fewer stressors (mean =0.61 and 0.55, respectively) than women residing in long-term moderate-poverty, long-term high-poverty and increasing poverty neighbourhoods (mean =0.81, 0.88 and 0.90, respectively).
Sample characteristics by neighbourhood poverty history, the Geographic Research on Well-being (GROW) Study (n=2726), weighted estimates*
Multivariable regression
We first considered results from logistic regression models predicting depressive symptoms (table 2). Women living in decreasing poverty neighbourhoods reported half the odds of depressive symptoms (Model 1; OR 0.5, 95% CI 0.3 to 0.8) compared with women living in long-term low-poverty neighbourhoods, after adjusting for demographic characteristics. No other neighbourhood type was associated with depressive symptoms. These findings held following adjustment for SES (Model 2). Duration of residence was unrelated to depressive symptoms (Model 2) and did not moderate the relationship between neighbourhood poverty histories and depressive symptoms (Model 3).
Depressive symptoms and sense of control regressed on neighbourhood poverty histories, the Geographic Research on Well-being (GROW) Study (n=2726), weighted estimates†‡
Next, we examined results from linear regression models predicting sense of control. Adjusting for demographic characteristics in Model 1 (table 2), long-term moderate-poverty (b=−0.55, SE=0.07), long-term high-poverty (b=−0.88, SE=0.10) and increasing poverty (b=−0.64, SE=0.07) neighbourhoods were each associated with lower sense of control compared with long-term low-poverty neighbourhoods. Conversely, decreasing poverty neighbourhoods were associated with higher sense of control (b=0.12, SE=0.05) than long-term low-poverty neighbourhoods. The inclusion of women's SES attenuated the associations (for all but decreasing poverty neighbourhoods) by about two-thirds; however, all associations remained statistically significant (Model 2).
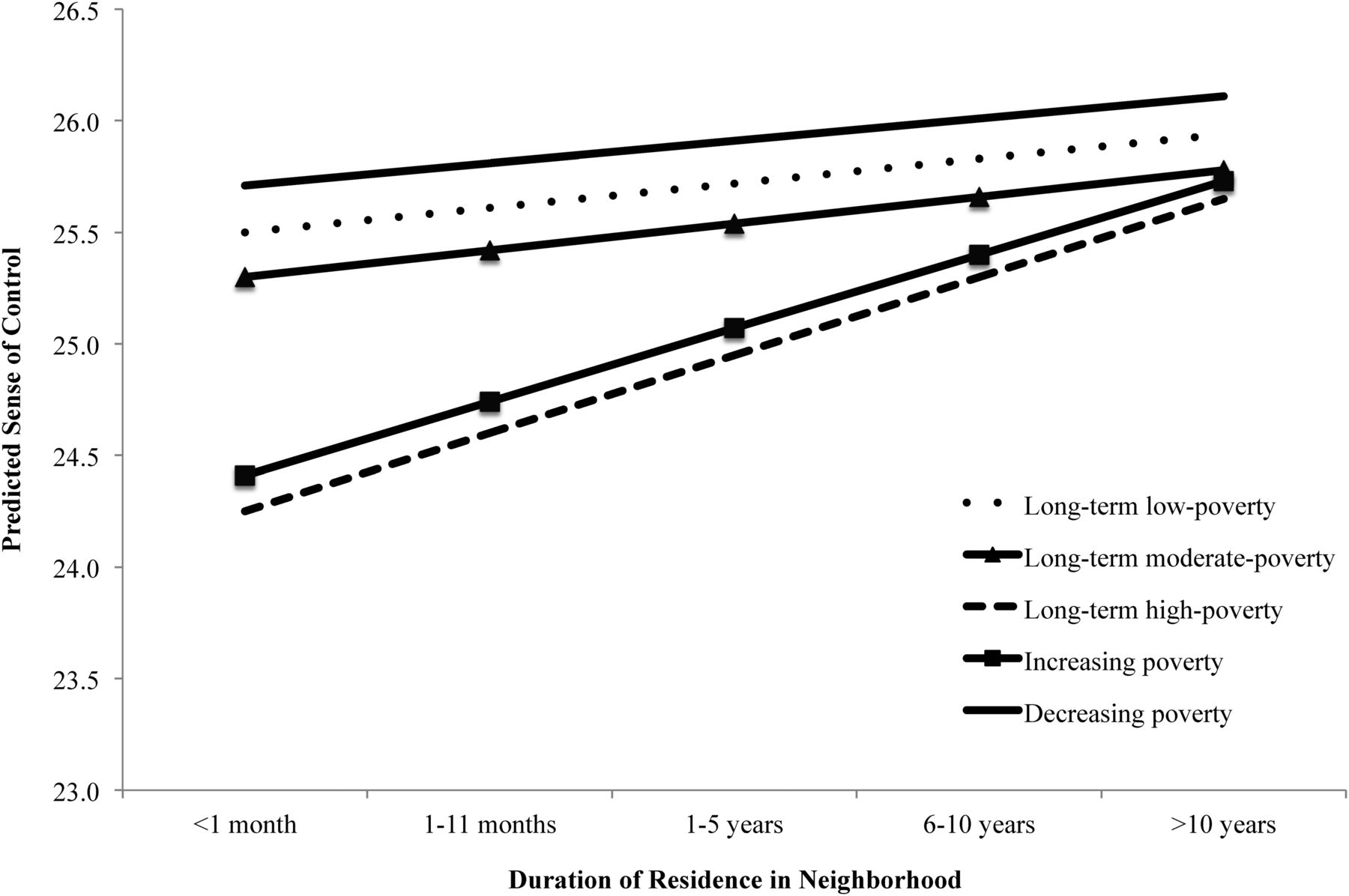
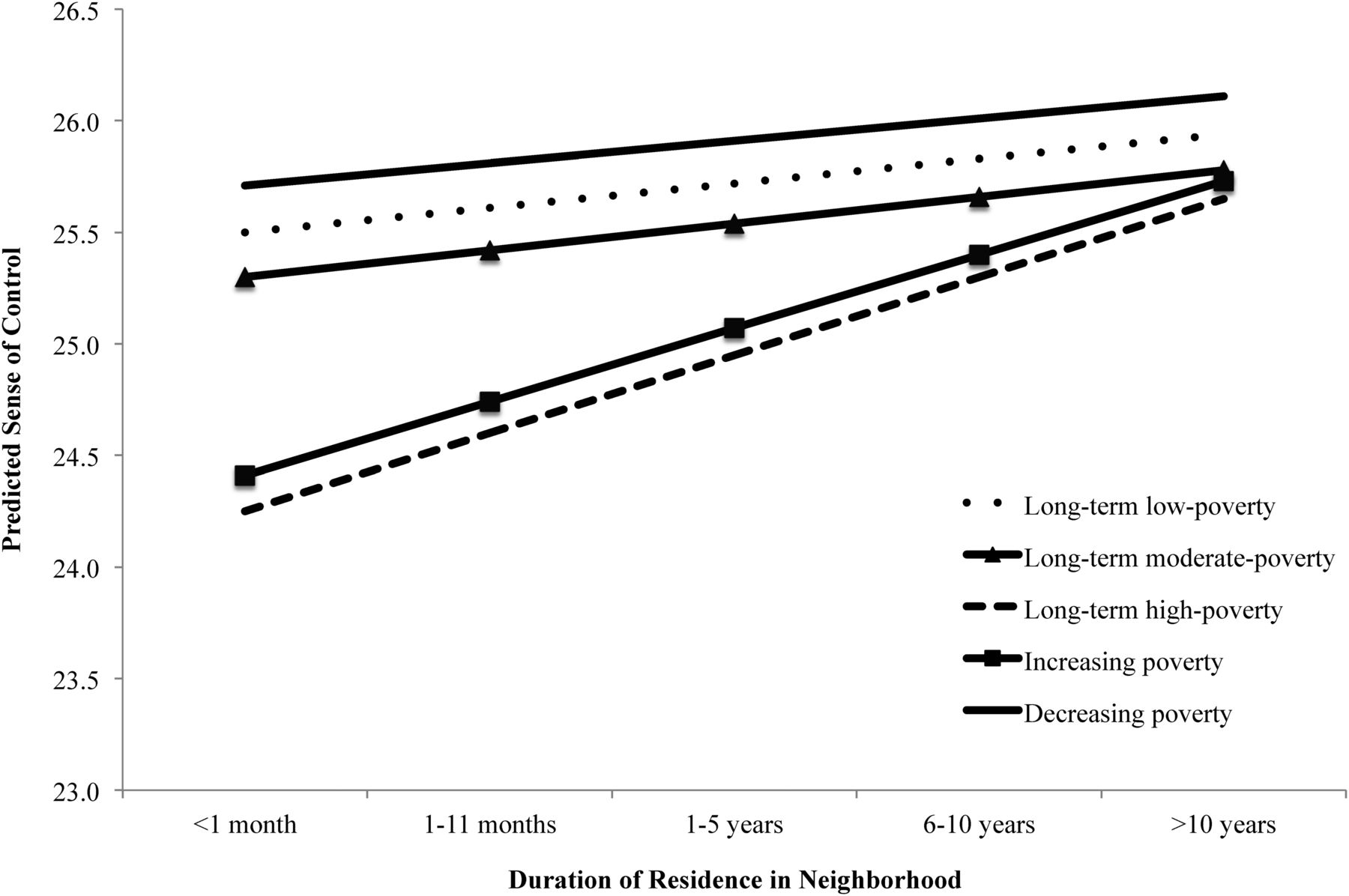
Longer duration of residence was associated with higher sense of control (b=0.22, SE=0.03; Model 2). The association between duration of residence and sense of control was stronger—and positive—for women residing in long-term high-poverty (b=0.24, SE=0.09) and increasing poverty (b=0.22, SE=0.07) neighbourhoods (Model 3). Figure 2 illustrates these findings; sense of control was lower for women residing in increasing and long-term high-poverty neighbourhoods compared with long-term low-poverty neighbourhoods at short durations of residence (<1 month), but were similar to long-term low-poverty neighbourhoods at long durations of residence (≥10 years).
{kind=link}
{kind=link}
Predicted sense of control by neighbourhood poverty histories and length of residence in neighbourhoods, GROW, n=2726. GROW, Geographic Research on Well-being Study.
Finally, we employed zero-inflated Poisson models to predict number of stressors (table 3). We found no association between the poverty histories of neighbourhoods and the log odds of never experiencing a stressor compared with experiencing at least one stressor (Inflate Model) or the expected log count of stressors (Count Model) in any model.
Number of stressors regressed on neighbourhood poverty histories, the Geographic Research on Well-being (GROW) Study (n=2726), weighted estimates†‡
Discussion
Significant attention has been paid to the influence of neighbourhood poverty on psychosocial well-being,1 ,3 ,29 yet few studies have considered the poverty histories of neighbourhoods. Using data from GROW, we investigated the relationship between the poverty histories of neighbourhoods and three indicators of psychosocial well-being—depressive symptoms, sense of control and number of stressors. We found evidence that the poverty histories of neighbourhoods matter for psychosocial well-being, but the extent to which they matter depends on the outcome under investigation.
Our hypothesis that women who resided in long-term high-poverty and increasing poverty neighbourhoods would be more likely to report depressive symptoms and experience a lower sense of control and more stressors compared with women residing in long-term low-poverty neighbourhoods was corroborated for sense of control, although not for depressive symptoms or number of stressors. Women residing in decreasing poverty neighbourhoods, however, were about half as likely to report depressive symptoms and had a greater sense of control than women residing in long-term low-poverty neighbourhoods. The null findings for number of stressors may be due to limited variation of these relatively rare events in our sample. Indicators of daily stressors, on the other hand, may be more responsive to neighbourhood conditions, but were unavailable in GROW.
Together, these findings offer a new prospect for policies or interventions aimed at improving the health of residents of high-poverty neighbourhoods. Prior efforts, such as the Moving to Opportunity Programme, relocated residents from high to lower poverty neighbourhoods, and had mixed results.30–33 Our findings suggest that policies and interventions that reduce neighbourhood poverty may result in positive psychosocial well-being for mothers residing in those neighbourhoods. In addition, psychosocial well-being was better among women living in decreasing poverty neighbourhoods compared with women living in long-term low-poverty neighbourhoods; it may be that experiencing positive neighbourhood change (in terms of lower poverty concentration) has an especially beneficial impact on psychosocial well-being.
We also hypothesised that longer residence in a neighbourhood would be associated with better psychosocial well-being but that this association would be weaker among women who resided in long-term high-poverty neighbourhoods compared with women who resided in decreasing or long-term low-poverty neighbourhoods. Contrary to expectations, we only found a moderating effect for sense of control, which translated into lower sense of control for women who had lived in long-term high-poverty and increasing poverty neighbourhoods for short durations (<1 month) but similar levels of sense of control for women residing in these neighbourhoods for long durations (≥10 years) compared with women in long-term low-poverty neighbourhoods.
Our results contrast with prior work documenting worse physical health outcomes with longer exposure to high-poverty neighbourhoods.13 ,14 For sense of control, brief exposure to high-poverty neighbourhoods may be detrimental because new residents have not yet developed the necessary strategies to respond to issues that arise from living in a high-poverty neighbourhood.34 Longer residence is associated with the development of social ties, greater social support and less financial stress.16 Thus, as residents develop these connections, their sense of control may improve. Alternatively, shorter residence in a neighbourhood may reflect greater residential instability, which may correlate with sense of control.
Our study includes a number of strengths. We traced the poverty histories of neighbourhoods across a 40-year period, accounted for women's duration of residence in their current neighbourhoods, and examined the role of neighbourhood poverty histories across three indicators of psychosocial well-being. Our study also has limitations. We were unable to trace the number of, or reasons for, women's residential moves, though we know how long they resided in their current neighbourhood. The meaning of residential stability may depend on age; that is, residential stability may yield different experiences for women who lived in their neighbourhood as children and adults (eg, young women) versus women who lived in their neighbourhoods only as adults (eg, mid-life women), even if the length of time spent in the neighbourhood is equivalent. Finally, given sample design, our findings are generalisable to mothers of infants residing in six counties in California in 2003–2007.
In sum, our study extends current neighbourhood and health research by investigating how changes or stability in neighbourhood poverty influences depressive symptoms, sense of control and stress. Our results suggest that policies aimed at reducing neighbourhood poverty may improve mothers' psychosocial well-being.
What this study adds?
Long-term high-poverty and increasing poverty neighbourhoods were associated with higher odds of depressive symptoms and a lower sense of control than long-term low-poverty neighbourhoods.
Decreasing poverty neighbourhoods were associated with lower odds of depressive symptoms and a greater sense of control than long-term low-poverty neighbourhoods.
Women who had resided in long-term high-poverty and increasing poverty neighbourhoods for short durations (<1 month) reported a lower sense of control but women residing in these neighbourhoods for long durations (≥10 years) had a similar sense of control compared with women in long-term low-poverty neighbourhoods.
Reducing neighbourhood poverty may improve mothers' psychosocial well-being.
What is already known on this subject?
Neighbourhood poverty is associated with poorer psychosocial well-being among residents.
Prolonged exposure to a neighbourhood may be beneficial or harmful for psychosocial well-being, depending on the neighbourhood condition being investigated.
References
Footnotes
Contributors KW and CC conceived the study. KH extracted and analysed the data. KW and SC drafted the manuscript. All authors critically reviewed the manuscript and approved the final version.
Funding This work was supported by a grant from the American Cancer Society (RSGT-11-010-01-CPPB) to CC and by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (5 R24 HD042849) to the Population Research Center at The University of Texas at Austin.
Competing interests None declared.
Ethics approval GROW was approved by the Institutional Review Boards at the University of Texas at Austin, the University of California, San Francisco and the California Department of Public Health; all participants gave informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.