Article Text

Abstract
Background The prevalence of metabolic diseases rises rapidly with an ageing population. Recent studies suggest the potential involvement of environmental chemicals in insulin resistance (IR) that plays a core role in the development of metabolic diseases. Polycyclic aromatic hydrocarbons (PAHs) are ubiquitous components of outdoor and indoor air pollution. The influence of PAHs on IR may differ depending on sex and weight.
Objectives We examined the association between exposure to environmental PAHs and IR in Korean urban elderly adults controlling for major risk factors that contribute to an increase in IR.
Methods Between 2008 and 2010, PAH metabolite levels (urinary 1-hydroxypyrene (1-OHP)) and the homoeostatic model assessment index (HOMA-IR) were repeatedly measured in 502 adults aged ≥60 years. Linear mixed effect models were fit to evaluate the associations of 1-OHP concentration with HOMA-IR. Subgroups were modelled by sex and weight.
Results After adjusting for sociodemographics, air pollution and metabolic disease status, the highest (vs lowest) quartile of 1-OHP was associated with an 0.57 (95% CI 0.10 to 1.04) increase in the HOMA-IR score (p trend=0.037). When stratified by sex, women presented a significantly dose-dependent trend of 1-OHP with HOMA-IR (p trend=0.013), whereas no association was observed in men (p trend=0.904). When further stratified by weight (body mass index ≥25 vs <25 kg/m2), a significant association was found only in overweight women (p trend=0.023).
Conclusions Our results suggest that environmental exposure to PAHs is associated with increased IR in elderly adults and that the association may be limited to overweight women.
- Biomonitoring
- Environmental epidemiology
- ELDERLY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Environmental pollutants are a worldwide public health issue affecting various health outcomes.1 Over recent years, the potential involvement of environmental chemicals in ‘metabolic diseases’ (eg, metabolic syndrome, diabetes mellitus (DM), cardiovascular disease and obesity) is of particular concern in the research community2 ,3 because of the increasing prevalence of metabolic diseases. Despite the extensive investigation of metabolic diseases, responsible mechanisms and a causative role of chemicals have not been fully elucidated.4 Hectors et al suggested that the implication of environmental chemicals in contributing to metabolic diseases may provide novel preventive strategies different from traditional methods, including lifestyle modification. They also emphasised the need for research on the link between environmental chemicals and insulin resistance (IR)2 because of IR's core role in the development of metabolic diseases.4–6
The polycyclic aromatic hydrocarbons (PAHs) and their derivatives are known to be carcinogenic and mutagenic7 and to be associated with an increase in oxidative stress.8 PAHs are ubiquitous components of outdoor air pollution (from motor vehicles, generation of electricity and residential heating) and of indoor air pollution (from environmental tobacco smoke (ETS) and cooking fumes).9 ,10 In East Asian (ie, Korean and Japanese) cities, major sources were in traffic exhaust and industrial production. Transboundary air pollution from neighbouring countries such as China also accounts for considerable amounts of PAHs.11 Several East Asian studies reported that PAHs are present chiefly in atmospheric particulate matter (PM).12–14 A Chinese study of five cities observed high PAH concentrations in an urban background and suggested that 90% of the total PAHs in ambient air were bound to PM2.5.12
While obesity is known to be inter-related with other metabolic conditions, the prevalence of obesity in the Asia-Pacific region is low compared with that in Europe and North America, although diabetes and metabolic syndrome are commonly experienced by Asians.15 ,16 Thus, identification of factors such as environmental chemicals that may trigger IR development would be particularly important for Asian people.
Given the ubiquitous high levels of PAHs in East Asian cities and the fact that IR is a central mechanism in the development of metabolic diseases, we focused on PAHS as potentially responsible for elevated IR. Owing to a report that women are more susceptible to the influence of PAHs17 and that obesity modifies associations between air pollution exposures and metabolic diseases,18 ,19 this study aimed to investigate the associations between IR and exposure to environmental PAHs and to evaluate the influences of sex-dependence and body weight-dependence in a longitudinal panel of elderly adults in Seoul.
Methods
Study participants
This study is a part of the Korean Elderly Environmental Panel (KEEP) study. Between August 2008 and August 2010, 560 non-institutionalised elderly adults (60 years of age or more) who regularly attended the Seongbuk-gu Community Center in Seoul were invited to participate in the study. Information on sociodemographic, environmental and behavioural factors and medical history was obtained at the time of enrolment. Participants underwent physical examination and laboratory testing at each follow-up visit (visits ranging from 1 to 5; 152, 70, 138, 124 and 76 participants visited 5, 4, 3, 2 and 1 times, respectively).
Of the initial 560 eligible participants (1856 observations), those lacking data regarding IR measures (n=14), urinary metabolites (ie, PAHs and cotinine; n=9), sociobehavioural factors (ie, education and physical activity; n=18), air pollution (n=23) and medical history (n=18; 9, 6, and 12 for diabetes, hypertension and cholesterol only) were excluded from the analysis, leaving a total of 502 individuals (996 observation).
Urinary metabolites
Participants came to the study centre between 10:00 and 12:00 at every visit. Spot urine samples, collected from each participant, were shipped to the NeoDIN Medical Institute (Seoul, Korea) for storage at −20°C until laboratory analysis.
PAHs exposure was estimated by measuring concentration of urinary 1-hydroxypyrene (1-OHP, CAS 5315-79-7, metabolite of pyrene), a biomarker commonly used to indicate the extent of short-term exposure to PAH.20 The elimination half-life of urinary 1-OHP was estimated to be 3.9 h.21 1-OHP was measured using a high performance liquid chromatograph (HPLC) system (Agilent 6410 triple Quad LCMS; Agilent, Santa Clara, California, USA) with a fluorescence detector (Model FP-2020; JASCO.co., Tokyo, Japan).22
The lower limit of detection (LODL) was 0.004 µg/L. At baseline, 1.59% of study participants had 1-OHP concentrations below the LODL.
Exposure to tobacco smoke was estimated using urinary cotinine concentration; metabolites were determined using urine cotinine test strips (Accutest NicAlert Strip; Jant Pharmaceutical Co., Encino, California, USA). The detection range for cotinine was 1–10 000 µg/L. At baseline, 31.7% of study participants had cotinine concentrations below the LODL, and 0.8% had concentrations above the upper LOD (LODU).
For urinary metabolites of 1-OHP and cotinine, those values below the LODL were imputed a value of LODL/2, and those over the LODU were imputed a value of LODU×2. Metabolite measurements were creatinine (Cr) corrected by dividing 1-OHP and cotinine concentrations by urinary Cr concentration (1-OHP/Cr and cotinine/Cr µg/g) in order to capture variation in urine concentration.23
Insulin resistance
Overnight fasting serum samples were collected and sent to the laboratory (NeoDIN Medical Institute) for storage at −70°C until analysis. The fasting blood glucose (FBG) level was determined by the hexokinase method using a Pureauto S GLU kit (Daiichi Pure Chemicals, Tokyo, Japan), and fasting insulin level by the double-antibody batch method using radio immunoassay (Elecsys Insulin and Elecsys 2010 Immunoanalyzers, Roche Diagnostics, Mannheim, Germany).
IR was then estimated by determination of the homoeostatic model assessment (HOMA-IR) score using the equation developed by Matthews et al24: HOMA-IR score=(fasting insulin level in µU/mL×FBG level in mmol/L)/22.5.
Covariates
We considered age, sex, education, physical activity, overweight, hypertension, DM, cholesterol level, exposure to tobacco smoke and to ambient PM ≤10 μm in diameter (PM10), and the length of time elapsed from the first visit as potential confounders. Covariates to be controlled were identified a priori, based on biological consideration and the literature review.25–27
Education was self-identified (≤elementary school, ≤high school, higher). Physical activity was defined as moderate to vigorous leisure activity versus none (yes/no).
Exposure to active and passive tobacco smoke was determined using urinary cotinine (log-transformed for normalisation; continuous). Exposure to ambient air pollution was estimated by daily mean levels of PM10 on the day immediately prior to an examination visit (continuous), using data from the monitoring site closest to each participant's residence, obtained from the Korea National Institute of Environmental Research (NIER, Incheon, Korea).
Body mass index (BMI) was computed as weight in kilograms divided by height in metres squared (kg/m2); overweight was defined as BMI ≥25 kg/m2 (yes/no). High-density lipoprotein cholesterol level (HDL-C) was defined according to whether it was lower or higher than the threshold value of 40 mg/dL for men and 50 mg/dL for women (low/high). Hypertension was defined as an average systolic blood pressure ≥140 mm Hg; diastolic blood pressure ≥90 mm Hg; self-reported physician diagnosis; or the use of antihypertensive medication (yes/no). DM was defined as FBG ≥100 mg/dL; self-reported physician diagnosis or the use of medication including antihyperglycaemic agents or insulin therapy (yes/no).
Statistical analysis
All statistical analyses were performed using SAS V.9.3 software (SAS Institute Inc, Cary, North Carolina, USA). Multivariate analysis using the linear mixed effect models was performed to estimate the effects of urinary 1-OHP concentrations on glucose level, insulin level and HOMA-IR score. Because 1-OHP metabolite was right-skewed, we used natural log-transformed levels to normalise the data. The influence of potential confounders was identified by the development of five sequential models: (1) model A adjusted for demographic factors (age, sex) and the time elapsed from the first visit; (2) model B adjusted for model A variables plus sociobehavioural factors (education, physical activity); (3) model C adjusted for model B plus ambient exposures (tobacco smoke, PM); (4) model D adjusted for model C plus metabolic syndrome components (overweight, hypertension, DM, HDL-C) and (5) model E adjusted for model D minus DM. In all models, we used a random intercept and a slope for the duration of time from the study baseline to account for the heterogeneity across subjects and subject-specific variability of IR over time. Follow-up observations were weighted to capture potential selection bias from the loss to follow-up by imputing the inverse predicted probability of having a follow-up response.28–30
We also modelled quartiles of 1-OHP. Values of 1-OHP concentration for all observations were categorised into four groups using the cut-off values for each quartile for 1-OHP concentration at the first visit (0.0753, 0.1237 and 0.2039 µg/g Cr). The models of 1-OHP quartiles with HOMA-IR were evaluated in all participants and subgroups stratified by sex (men vs women) and weight (BMI ≥25 vs <25 kg/m2). We estimated the change in HOMA-IR by comparing each of the upper three quartiles with the lowest quartile (reference).
We conducted sensitivity analyses for those who did not have abnormal liver function and for subgroups stratified by the presence of DM. We set the cut-off values for elevated aspartate aminotransferase, alanine aminotransferase and γ-glutamyl transferase at 35, 45 and 60 IU/L, respectively. Then we set the criteria for clinically significant abnormality for liver function test as >1.5 times the cut-off value of any one of the liver enzymes.31
Results
A total of 502 individuals (132 men and 370 women) were included in the final study population. Compared with individuals excluded, those included reported no significant differences regarding any variable except a diagnosis of current hypertension (see online supplementary table S1). Table 1 shows the general characteristics of the study participants at enrolment. Overall, the means of age and HOMA-IR were 70.8 (±SD 5.3) years and 1.7 (±1.7). The geometric mean of urinary 1-OHP was 0.12 (95% CI 0.11 to 0.13) µg/g Cr. Women were more likely to be less educated and more exposed to ambient PM10 and more likely to have higher BMI, higher fasting insulin levels, lower cotinine levels and low HDL-C.
General characteristics (mean±SD) at enrolment (n=502)
Table 2 presents distributions of the three IR measures by quartiles of urinary 1-OHP concentration. Female participants with higher 1-OHP levels were more likely to have higher HOMA-IR. No significant pattern by 1-OHP levels was found in male participants.
Characteristics of study population by urinary 1-OHP quartile
Table 3 shows estimated associations between urinary 1-OHP concentration, as a continuous variable, and glucose level, insulin level and HOMA-IR score in different covariate-adjusted models. 1-OHP concentration was positively associated with HOMA-IR score in all models with borderline significance. Adjustments made in models B, C and D did not alter those associations. In the fully adjusted model (model D), a unit increase of log-transformed 1-OHP was significantly associated with a 0.16 (95% CI 0.00 to 0.31) score increase in HOMA-IR. When subtracted DM from a fully adjusted model, their association was similar but less significant (see model E). In all of the following analyses, we used the model E because development of DM is highly correlated with IR and controlling for such a DM may result in over-adjustment.
Regression coefficients (β (95% CIs)) for change in glucose, insulin and HOMA-IR score by a unit increase in ln-transformed urinary 1-OHP
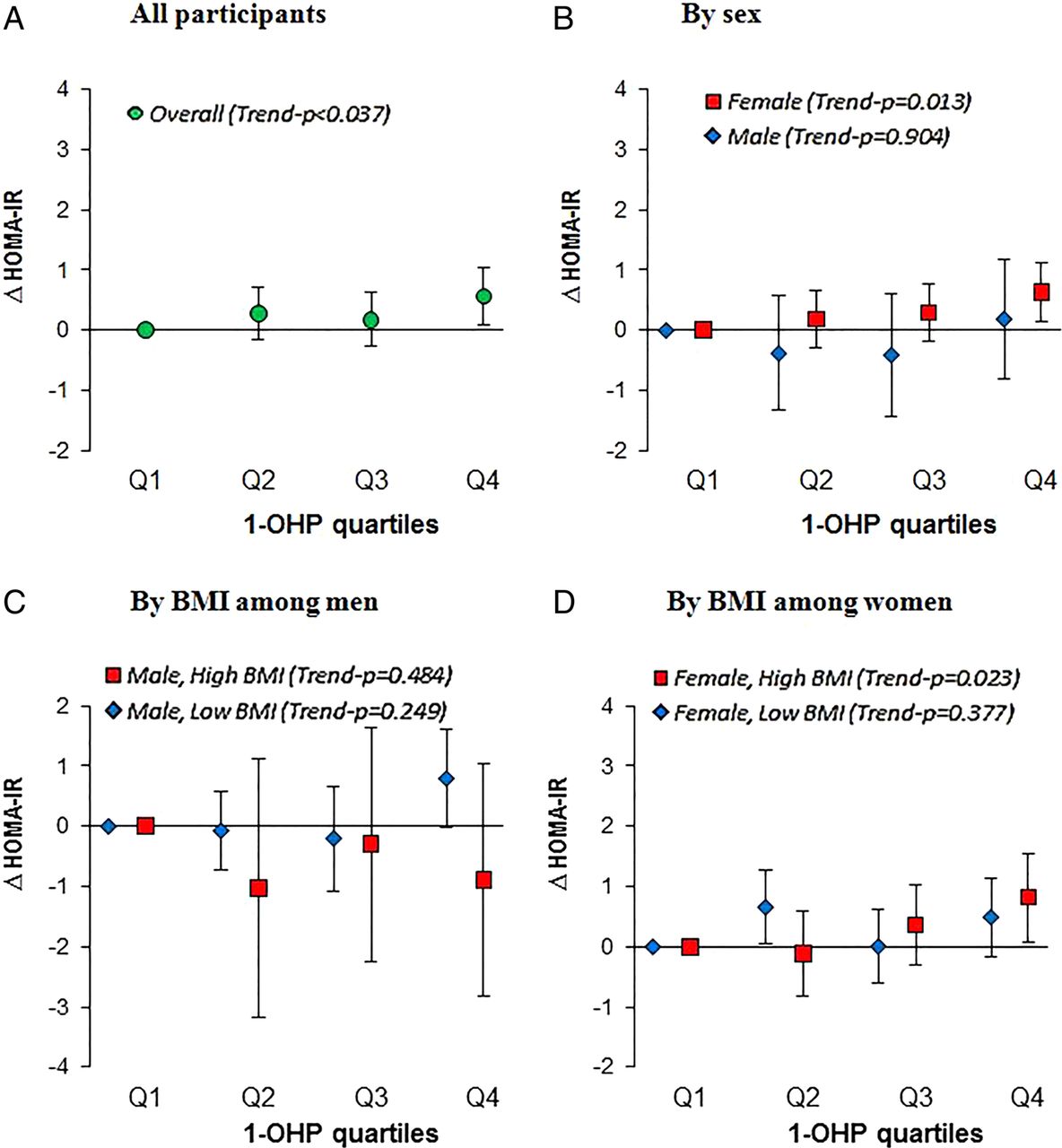
Figure 1 (online supplementary table S2) shows the estimated changes in HOMA-IR with urinary 1-OHP concentration as quartiles. Overall, there was a significant trend of 1-OHP quartiles with HOMA-IR (p=0.037). After controlling for potential confounders, individuals in the highest quartile (1-OHP >0.204 µg/g Cr) had 0.57 (95% CI 0.10 to 1.04) higher HOMA-IR scores than those in the lowest quartile. We also evaluated associations of HOMA-IR with urinary 1-OHP as quartiles in four groups stratified by a combination of sex and overweight (BMI ≥25 kg/m2 or not). In particular, overweight women presented a significant trend of 1-OHP with HOMA-IR (p=0.023), whereas no trends were observed in men and non-overweight women.
{kind=link}
Fully-adjusted changes (95% CI) in HOMA-IR score in relation to 1-OHP quartiles (quartile 1 is reference) in (A) overall participants, (B) different sex, and in subgroups stratified by overweight in (C) men and (D) women. Values were adjusted for age, sex, elapsed time, education, physical activities, BMI, hypertension, HDL-cholesterol, cotinine, and ambient PM10. Overweight was defined as BMI≥25kg/m2. 1-OHP quartiles cut-off points: 0.0753, 0.1237, 0.203 µg/g Cr” BMI, body mass index; 1-OHP, 1-hydroxypyrene; HOMA-IR, homoeostatic model assessment of insulin resistance)
Owing to a possibility that poor functional enzymes in the liver may increase IR and delay metabolism of PAHs, we evaluated associations of HOMA-IR with urinary 1-OHP in the study population that excluded participants who had abnormal liver function (see online supplementary table S3). However, this exclusion did not alter our findings. We also conducted subgroup analyses stratified by the presence of DM and found an enhanced effect of 1-OHP on HOMA-IR in individuals with DM, whereas we did not observe the significance in the relations in those without DM (see online supplementary table S4).
Discussion
In this panel study of urban elderly adults in Korea, environmental exposure to PAHs was associated with increased IR, even after adjusting for sociodemographic factors and potential risk factors including other environmental exposures and metabolic conditions. In addition, the present data suggest that the influence of PAHs exposure may be limited to overweight women.
To the best of our knowledge, this is the first investigation to examine dose–response associations between IR and PAHs. We found that log-transformed concentrations of urinary 1-OHP reflecting PAHs were positively correlated with HOMA-IR scores with borderline significance. Categorical analysis of 1-OHP modelled as quartiles yields a significant dose–dependent trend with elevated HOMA-IR. Several epidemiological studies suggested that elevated oxidative stress is related to increased PAHs exposure.8 ,32 A recent study of 1333 male coke oven workers monitored the levels of environmental PAHs and oxidative biomarkers and indicated significant dose-related increases in oxidative damage to DNA and lipids with urinary metabolites (1-OHP) and plasma adducts (BPDE-Alb) of PAHs.32 Another study of 120 Korean schoolchildren reported a significant association of urinary 1-OHP with an oxidative stress biomarker using urinary malondialdehyde (MDA).8 These reports could provide useful biological interpretation of our finding an association between urinary 1-OHP and IR. In fact, we examined associations between urinary 1-OHP and MDA levels and were able to confirm a significant relationship (online supplementary table S5) consistent with those from previous studies. From the observation that 1-OHP is positively associated with oxidative stress and that oxidative stress may be involved in IR pathogenesis,33 the associations of PAHs with IR may be explained by a pathway in which oxidative stress is increased by PAHs exposure.
Another possible explanation for the observed associations of PAHs with IR is that PAHs are potentially related to oestrogenic activity,34 ,35 a relationship that could mediate the effect of PAHs in development of IR. In our analysis, when modelled subgroups stratified by sex, a significant dose–dependent association for PAHs with IR was observed in women only, but not in men. Previous research has suggested that the correlation of fasting glucose and insulin is greater with the oestradiol/testosterone ratio than with oestradiol or testosterone alone.36 Since the oestradiol/testosterone ratio is higher in women, even old women, than in men, these research suggestions support our finding that women are susceptible to the influence of oestrogen-like PAHs on IR.
We also examined subgroups further stratified by weight. Overweight women were observed to have a significant association of HOMA-IR with PAHs exposure, whereas men and non-overweight women had no significant associations. The weight-dependent effects are consistent with previous studies indicating obesity as an effect modifier on the associations of air pollution and metabolic diseases.18 ,19 It is still unclear how weight modifies the relationship between PAHs exposure and IR in women. Overweight may cause metabolic disturbance in itself via oxidative stress/oestrogenic activity,18 ,19 which may potentially act in an additive manner with PAHs exposure, particularly in sensitive women.
Casals-Casas and Desvergne suggest a ‘metabolic disruptor hypothesis’, that is, the potential involvement of environmental chemicals in metabolic disease aetiology.37 Since the worldwide prevalence of diabetes and metabolic syndrome has been increasing with an ageing population, identifying non-traditional risk factors for metabolic diseases could provide a better strategy than traditionally known factors, and many researchers emphasise the need to understand the particular role of environmental chemicals in the development of IR.2 ,3 Owing to this context, our study focused on PAHs, a ubiquitous environmental chemical with potential risk, and our findings suggest that exposure to PAHs contributes to the development of IR, after adjusting for traditional risk factors.
The current study suggests that even low-level exposure to environmental PAHs observed in an urban population is associated with IR and so supports efforts to reduce current levels of environmental PAHs. Compared with participants in the lowest quartile, those in the highest quartile of urinary 1-OHP (0.204–4.461 µg/g Cr) are at risk for significantly higher IR. Unfortunately, there is no standard for acceptable concentrations of urinary 1-OHP resulting from PAHs exposure, although the US Environmental Protection Agency (EPA) has designated 32 PAH compounds as priority pollutants.38 A recent report using data from the Korean National Environmental Health Survey, a representative sample of Korean adults aimed at estimating nationwide environmental exposures, showed that the national geometric mean of urinary 1-OHP was estimated to be 0.15 (95% CI 0.05 to 0.25) µg/g Cr.39 Therefore, our findings show that a considerable number of Korean adults may be exposed to PAHs in ranges of risk. The primary sources of PAHs producing high 1-OHP concentrations are motor vehicles, generation of electricity and residential heating of outdoor air; ETS and cooking of indoor air; and burned food of dietary intake in the general population.9 ,10 ,40
This study also examined associations between IR and other PAHs biomarker (urinary 2-naphthol) but failed to observe a meaningful relationship (data not shown), although 2-naphthol is known to be highly correlated with exposure to PAHs specific to tobacco smoking.41 Our observations of 1-OHP but not of 2-naphthol associations suggest that PAHs responsible for IR may not have their source in tobacco smoke but from other exposures (eg, air pollution from motor vehicles and heating, grilled foods). Further investigation in a large general population is required, however, to elucidate the source-dependent role of PAHs for IR.
The main strengths of this study include (A) the adjustment for potential confounders of traditional risk factors including environmental exposures as well as metabolic conditions, which enabled us to observe independent effects of PAHs exposure in IR; (B) the repeated measures design of the panel study, which enabled the capture of between-subjects and within-subjects variations and (C) the use of short-term biomarkers from each participant for PAHs exposure and IR outcome that accounted for variation in individual daily levels.
Several limitations must be considered in interpreting the results. First, because of the nature of cross-sectional measures, our results may not necessarily indicate a causative role for PAHs exposure in elevating IR. Second, given that the number of participants is not large enough to observe a statistically reliable finding; our finding with borderline significance would be improved when the sample size is bigger. Third, this study used HOMA-IR score, a surrogate marker to evaluate IR. One might argue, therefore, that HOMA modelling may be less accurate than direct measures using the gold standard method (ie, the glucose clamp technique),42 and HOMA-IR response may be altered on patients with DM treated with insulin.43 In fact, we observed an enhanced effect of 1-OHP on IR in DM-diagnosed participants while we did not find a significant relationship in the participants excluding patients with DM. However, a simpler tool, HOMA-IR, may be more appropriate for use in large-scale epidemiological studies43 ,44 such as this study with repeated measures within subjects, although the gold standard is a good tool for intensive physiological studies. The HOMA-IR score is strongly correlated with the gold standard-IR and has proved to be a robust epidemiological tool for IR assessment.45 In addition, most of the study subjects with DM may be managed by oral antihyperglycaemic agents or lifestyle change (ie, diet, exercise) without insulin treatment (see online supplementary text). Several studies also support that HOMA-IR is a useful method to evaluate insulin sensitivity even in patients with DM treated with insulin.46 ,47 Nevertheless, our observation on enhanced effect in patients with DM still needs to be interpreted carefully. Fourth, we cannot rule out selection bias in finding the association between PAHs and IR, which may be different for participants included in our analysis and those excluded (for absence of information). The included participants were more likely to have hypertension than those excluded (see online supplementary table S1). In sensitivity analysis for subgroups by diagnosis of hypertension, a stronger influence of 1-OHP on IR was found in hypertension-diagnosed participants than in non-diagnosed participants, although the difference was only marginally significant (data not shown). We expect, therefore, that associations in the excluded participants and/or in a general population may be smaller than our observed effect.
In conclusion, this study supports the contention that exposure to environmental PAHs currently observed in the Korean urban elderly is a risk factor for development of IR, independent of traditionally known risk factors, and that its risk may be limited to women, particularly overweight women, suggesting sex-dependent and body weight-dependent effects. Given the increasing prevalence of metabolic disease, efforts in reducing exposure to environmental PAHs is important for improving public health.
What is already known on this subject
Recent studies suggest the potential involvement of environmental chemicals in insulin resistance, which plays a core role in the development of metabolic diseases.
Polycyclic aromatic hydrocarbons (PAHs) are ubiquitous environmental chemicals of outdoor and indoor air pollution, with a potential risk of elevated oxidative stress.
To the best of our knowledge, there has been no investigation to examine dose–response associations between insulin resistance and PAHs.
What this study adds
The exposure to environmental PAHs currently observed in the Korean urban elderly is associated with increased insulin resistance.
The association is limited to overweight women, suggesting sex-dependent and body weight-dependent effects.
Given the prevalence of metabolic disease, efforts in reducing exposure to environmental PAHs is important for improving public health.
Acknowledgments
KM Kim, GH Cho and YM Choi were responsible for interviewing participants and cleaning the collected data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors Y-HC and Y-CH designed the study; JHK acquired the data; Y-HC analysed data and wrote the manuscript; Y-CH critically revised the manuscript.
Funding This work was supported primarily by the Susceptible Population Research Program (0411-20080013, 0411-20090007, 0411-20100016) from the Korea Ministry of Environment, and the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Korea Ministry of Education (2012018364 and 2013R1A6A3A04059556).
Competing interests None.
Patient consent Obtained.
Ethics approval This study was approved by the Institutional Review Board of Seoul National University Hospital/College of Medicine (IRB no. H-0804-045-241).
Provenance and peer review Not commissioned; externally peer reviewed.