Article Text

Abstract
Background Evidence of an association between fine particulate matter (PM2.5) and morbidity is limited in Asia. We used a case-crossover design to evaluate the association between short-term exposure to PM2.5 and emergency ambulance dispatches (as a proxy of acute health outcomes), and to calculate the extent to which a 10 μg/m3 decrease in PM2.5 concentrations would reduce the number of ambulance dispatches.
Methods We used data on emergency ambulance dispatches in Fukuoka City, Japan between 2005 and 2010. Emergency ambulance services are publicly funded and cover the entire city. After excluding ambulance dispatches related to external injuries and pregnancy/childbirth, we analysed data on the remaining 176 123 dispatches. We also collected records of daily concentrations of PM2.5 from one ambient air pollution monitoring station. ORs per 10 μg/m3 increase in PM2.5 were estimated using conditional logistic regression controlled for ambient temperature and relative humidity.
Results During the study period, the average daily concentration of PM2.5 was 20.3 μg/m3. Exposure to PM2.5 was associated with emergency ambulance dispatches in general (lag0–1; OR=1.008 (95% CI 1.002 to 1.014)) and with dispatches due to respiratory diseases (lag0–1; OR=1.027 (1.007 to 1.048)). No association was observed for dispatches due to cardiovascular diseases. We estimated that a 10 μg/m3 decrease in PM2.5 concentrations would have led to approximately 260 (estimated range=70–460) fewer ambulance dispatches in Fukuoka for 2012.
Conclusions Providing further evidence on the short-term health effects of PM2.5 exposure, we found that exposure was associated with an increased number of emergency ambulance dispatches. The effect was, however, relatively small.
- AIR POLLUTION
- Environmental epidemiology
- ENVIRONMENTAL HEALTH
Statistics from Altmetric.com
Introduction
There is growing evidence that exposure to particulate matter harms human health,1 even though the effects may seem relatively small in comparison with those of major risk factors like smoking. However, as more and more populations are exposed to particulate matter, it is becoming a global public health burden. A systematic analysis for the Global Burden of Disease Study 2010 put fine particulate matter (PM2.5, ie, fine particulate matter collected with a sampler with a 50% cut-off point of 2.5 µm) in the top 10 causes of disease burden worldwide, accounting for 3.2 million deaths in 2010.2
There is limited evidence on the health effects of PM2.5 exposure in Japan, because air quality standards were based on suspended particulate matter measurements (particles with diameters of less than 10 μm) until PM2.5 was added as a criterion in 2009. In other Asia countries, evidence of an association between exposure to PM2.5 and morbidity is also more limited than it is in Europe and the USA. It is also clear from the literature that epidemiological evidence collected in Western countries cannot necessarily be extrapolated to Asian populations. In addition, the health effects of PM2.5 have been reported to differ according to its chemical composition, which is affected by geographic location.3 Therefore, the health effects of PM2.5 exposure needs further study in Asia. In Japan, this association has become a matter of national concern because of high concentrations found in air pollution drifting periodically into the country from other East Asian nations recently.4 ,5 Information on the short-term health effects of PM2.5 that are closely connected to everyday life is urgently needed.
The purpose of the present time-stratified case-crossover study was to examine whether short-term increases in PM2.5 concentrations are associated with the number of emergency ambulance dispatches in Japan. There is precedent for using ambulance dispatch data to examine the health effects of PM2.56 ,7; such data are helpful in assessing acute health events related to respiratory and cardiovascular diseases, which are the main focus of epidemiological studies on PM2.5. Quantification of the public health impact of PM2.5 exposure is important, so we also calculated the extent to which a 10 μg/m3 decrease in PM2.5 concentrations would reduce the number of ambulance dispatches.
Materials and methods
Study area
This study was carried out in Fukuoka City, Fukuoka Prefecture, one of the biggest cities in Japan (see online supplementary figure), with a population of approximately 1.5 million, and a moderate climate (average annual temperature c.17°C). Fukuoka is in Kyushu (130°24′E, 33°35′N), the closest of Japan's main islands to the Asian continent, making it susceptible to transboundary air pollution.4 ,8 Owing partly to this susceptibility, PM2.5 concentrations in Fukuoka are relatively high compared with other Japanese cities; the range of daily mean concentrations is also wide.9
Environmental data
We obtained data on PM2.5 from Fukuoka City. The tapered element oscillating microbalance (TEOM) method was used to measure hourly concentrations of PM2.5 almost every day during the 2191-day study period (measurements were unavailable for 1.3% of the total days) at one ambient air pollution monitoring station selected as representative of the urban background in Fukuoka, and daily mean concentrations were calculated. TEOM measurements correlate well with those obtained by the federal reference method.10
Data on other pollutants (nitrogen dioxide (NO2), photochemical oxidants (Ox) and sulfur dioxide (SO2)) were obtained from the National Institute for Environmental Studies’ atmospheric environment database. Ox is defined as mixtures of ozone and other secondary oxidants generated by photochemical reactions, and is considered to be a proxy for ozone. Hourly data from eight monitoring stations in Fukuoka were collected, and daily mean concentrations of NO2 and SO2 were calculated across the monitoring stations, along with average daily maximum 8 h mean concentrations of Ox.
Meteorological data were obtained from the Japan Meteorological Agency. Hourly measurements were used to calculate daily mean ambient temperatures and relative humidity. Data on weekly influenza incidence were obtained from the Japan National Institute of Infectious Diseases. Influenza epidemic week was defined as the week when the weekly number of influenza cases was above the 90th centile of distribution during the study period or not,11 so influenza was a dichotomised variable as epidemic week or not.
Information on emergency ambulance dispatches
In Japan, emergency medical services are provided free of charge by local governmental fire defence headquarters,12 ,13 and citizens can call ambulances via the emergency number 119.
We obtained data on 307 711 emergency ambulance dispatches covering the entire city of Fukuoka between 1 January 2005 and 31 December 2010. After excluding dispatches related to external injuries and pregnancy/childbirth, we were left with data on 176 123 dispatches (57.2%) for analysis. Records of the initial diagnoses made at the emergency departments where the transported patients were treated were used to code the causes of the ambulance dispatches according to the International Classification of Diseases, 10th revision (ICD-10); one medical doctor (TM) did the coding. Since there is evidence of an association between PM2.5 and cardiopulmonary diseases,1 we defined ambulance dispatches related to respiratory diseases (ICD-10: J00-99) and cardiovascular diseases (ICD-10: I00-99), which accounted for 9% (n=15 857) and 18.1% (n=31 837) of the total, respectively, as cause-specific. The ratio of ambulance dispatches due to respiratory and cardiovascular diseases was similar to that found in an earlier study in another Japanese city.14
We submitted the study protocol to the Ethical Review Board of the National Institute for Environmental Studies for approval but were told by the Board that approval was not required because the study data did not include individual identifiers.
Statistical analyses
The case-crossover design used in this study was developed to assess the acute effects of transient exposure. The design has the ability to control for time-invariant characteristics such as age and sex, because within-subject comparisons are made between case periods and control periods. Case periods in this study were defined as the days of emergency ambulance dispatches, and the control periods (3–4 per case) were selected on corresponding days of the week within the same calendar month. For example, if an ambulance was dispatched on 15 October, four control days were assigned: 1, 8, 22 and 29 October. This control selection strategy is called ‘time-stratification’, and is designed to adjust for time-dependent confounding within strata-time by methods.15
Conditional logistic regression models were used to estimate the adjusted ORs and 95% CIs of emergency ambulance dispatches associated with 10 μg/m3 increases in PM2.5 concentrations, after including the mean ambient temperature (a natural spline with 4° of freedom) and relative humidity from the case day (lag0) to 3 days prior (lag3). To evaluate the lag effect of PM2.5, we applied a lag-stratified distributed lag model,16 entering the average concentrations of PM2.5 during the case day (lag0) to 1 day preceding it (lag1) (lag0–1), during lag2–lag3 (lag2–3) and during lag4–lag6 (lag4–6) simultaneously. To confirm the robustness of PM2.5 effect estimates against potential confounding by NO2, Ox and SO2, we constructed two-pollutant models adjusted for the mean concentrations of each copollutant (lag0–3). Pearson's correlations coefficients between PM2.5 and the other pollutants were 0.43 for NO2, 0.41 for Ox and 0.60 for SO2 (see online supplementary table S1). Although these correlations by season were different, particularly regarding Ox, there was no statistical evidence in two-pollutant models that the association between PM2.5 and ambulance dispatches varied according to season. We also performed stratified analyses by age (0–19 years, 20–64 years and 65 years or older) and sex to examine the effects by subgroup, and a statistical check for interaction by age strata and sex using the likelihood ratio test. Similar analyses were repeated to investigate other pollutants. Furthermore, several sensitivity analyses were performed. First, because of possible bias in control selection, we excluded participants transported to hospitals on national holidays. Second, we investigated whether any association between PM2.5 and ambulance dispatches was detectable when PM2.5 concentrations were lower than those of air quality standards stipulated by the Japanese Ministry of the Environment17 and US Environmental Protection Agency18 (daily mean, 35 μg/m3), and by the WHO19 (daily mean, 25 μg/m3): analyses were restricted to participants exposed to PM2.5 concentrations below those values. Third, we additionally adjusted for influenza epidemics. And fourth, to check for possible confounding by the effects of prolonged low temperatures, a significant factor in respiratory disease,20 we adjusted for temperature at lag0–14.11
To illustrate the public health impact, we estimated the reduction in the number of annual emergency ambulance dispatches attributable to a 10 μg/m3 decrease in the daily PM2.5 concentrations. In accordance with a modified method for calculating the population attributable fraction,21 the annual reduction was defined as N×(OR–1)/OR, where N was the number of annual ambulance dispatches excluding those related to external injuries and pregnancy/childbirth. By multiplying the total number of ambulance dispatches by 0.572 (57.2%), we thus assumed approximately 33 000 ambulance dispatches in Fukuoka for 201222 as N. We also estimated the corresponding reduction in administrative expenditure based on a rate of 7600 Japanese yen per ambulance dispatch23 and using exchange rates of 100 yen=$1=€0.7.
All statistical analyses were performed with Stata V.11 (Stata Corporation, College Station, Texas, USA), and statistical tests were two-tailed with significance levels set at p<0.05.
Results
Of the 176 123 emergency ambulance dispatches investigated, 9.3% were for persons aged 0–19 years, 45.3% for people aged 20–64 years and 45.4% for people aged 65 years or older; 86 127 dispatches (48.9%) were for men. A summary of meteorological factors and daily mean concentrations of air pollutants is shown in table 1. The average PM2.5 concentration over the study period was 20.3 μg/m3, and concentrations exceeded Japanese air quality standards on 211 days (9.8%).
Summary of meteorological factors and daily mean concentrations of air pollutants from January 2005 to December 2010 in Fukuoka, Japan
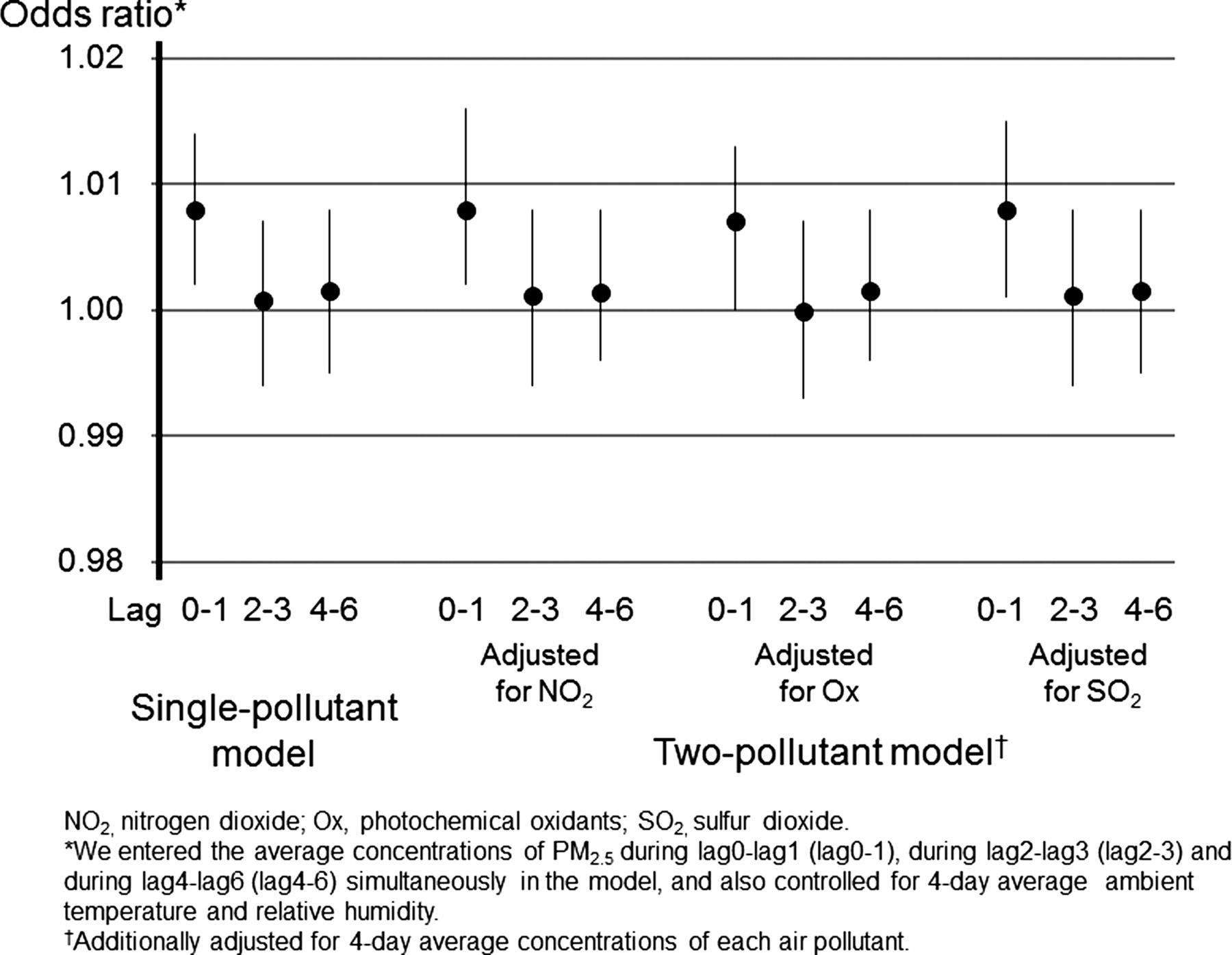
Figure 1 shows the association between PM2.5 exposure and emergency ambulance dispatches. PM2.5 exposure was associated with increased ambulance dispatches for lag0–1 (OR=1.008 per 10 μg/m3, 95% CI 1.002 to 1.014). When the subjects transported to hospitals on national holidays were excluded, similar results were obtained (OR=1.008, 95% CI 1.002 to 1.014). We restricted analyses to subjects exposed to PM2.5 concentrations below those stipulated by air quality standards. Although the point estimations changed slightly, those 95% CIs showed considerable overlap (OR=1.010 (95% CI 1.001 to 1.019) for ≤35 μg/m3, OR=1.007 (0.994 to 1.020) for ≤25 μg/m3). Including influenza epidemics in the model did not affect our results (OR=1.008, 95% CI 1.002 to 1.014; see online supplementary table S2). In the two-pollutant models, the OR estimates for lag0–1 were similar (figure 1). The OR for lag0–1 was used to calculate the reduction in annual ambulance dispatches attributable to a 10 μg/m3 decrease in daily PM2.5 concentrations. The estimated reduction was approximately 260 (estimated range=70–460) dispatches in Fukuoka for 2012, with a correspondingly reduced administrative expenditure of approximately 2 million yen (c. $20 000/€14 000).

{kind=link}
ORs (black circles) of emergency ambulance dispatches per 10 μg/m3 increase in fine particulate matter (PM2.5). Error bars indicate 95% CIs.
Table 2 shows the results of cause-specific emergency ambulance dispatches according to age strata and sex. PM2.5 (lag0–1) was associated with an elevated risk of ambulance dispatches due to all causes in those aged 65 years or older (OR=1.012 per 10 μg/m3, 95% CI 1.003 to 1.021) and in men (OR=1.011, 95% CI 1.002 to 1.020); however, no statistical evidence for interaction by age strata or sex was observed. In the cause-specific analyses, the OR for respiratory diseases was 1.027 at lag0–1 (95% CI 1.007 to 1.048) in the overall analysis. We confirmed the robustness of this finding by adjusting for temperature at lag0–14 (see online supplementary table S3). In contrast, we did not find any associations for cardiovascular diseases.
ORs and 95% CIs of cause-specific emergency ambulance dispatches per 10 μg/m3 increase in fine particulate matter (PM2.5) by age strata and sex
Table 3 presents the associations between other air pollutant concentrations and emergency ambulance dispatches. Exposure to copollutants was not associated with ambulance dispatches due to all causes. However, positive associations were observed between NO2 and SO2 concentrations and respiratory diseases for lag2–3, with estimated ORs of 1.047 per 10ppb (95% CI 1.005 to 1.091) and 1.196 per 10 ppb (95% CI 1.001 to 1.429), respectively. With regard to NO2, the statistically significant association was found in those aged 19 years or younger (OR=1.162, 95% CI 1.028 to 1.313).
Associations of other air pollutants with emergency ambulance dispatches
Discussion
Observed association between short-term exposure to PM2.5 and emergency ambulance dispatches was robust to adjustment for copollutants and was independent of influenza epidemics. An estimated increase in ambulance dispatches of 0.8% per 10 μg/m3 rise in PM2.5 appeared to be similar to that reported in an earlier case-crossover analysis of all-cause mortality in Fukuoka City,9 though different outcomes made it difficult to directly compare our results with the earlier findings. We found no statistical evidence of interaction by age strata. A recent meta-analysis presented the higher particulate matter (aerodynamic diameter ≤10 μm (PM10))-associated mortality risk in people aged 65 years or older,24 so further research into age-specific differences is needed. In this meta-analysis, a 10 μg/m3 increase in PM10 exposure was associated with 0.28% (95% CI 0.11 to 0.44) and 0.34% (95% CI 0.19 to 0.49) increases in risk of death for men and women, respectively.24 The overlap of 95% CIs means a less pronounced difference between men and women, suggesting consistency between our findings and the results of this meta-analysis.
As far as we know, this is the first study of the impact of exposure to PM2.5 on emergency ambulance dispatches. By our estimate, a 10 μg/m3 decrease in PM2.5 concentrations would have reduced the number of ambulance dispatches in Fukuoka by approximately 260 (estimated range=70–460) in 2012. As ambulance dispatches are not to be related to exposure to PM2.5 might remain in the all-cause dispatches, we should be cautious about possible overestimation. As our results show, the increased health risk of PM2.5 exposure is relatively small. However, since populations are aging rapidly all over the world, increasing vulnerability to PM2.5 exposure is expected. Japan has the longest life expectancy at birth worldwide, and the number of ambulance dispatches is estimated to exceed 6 million annually by 2023 or 2024.13 From the viewpoint of public health, the sheer number of people subject to PM2.5 exposure means that even a small increased health risk is likely to have a financial impact on the emergency ambulance system. The estimated association between PM2.5 exposure and ambulance dispatches tended to be similar when analyses were restricted to subjects exposed to PM2.5 concentrations below those stipulated in Japanese air quality standards, so efforts should be made to reduce PM2.5 exposure as far as possible.
With respect to cause-specific emergency ambulance dispatches, we observed an association between short-term PM2.5 exposure and increased risk for respiratory diseases. This finding is biologically plausible, because the respiratory system is the first system affected by contact with PM2.5; PM2.5 causes lung inflammation.1 Also, this does not contradict the results of past epidemiological studies. A study in Linz, Austria showed that exposure to PM2.5 tended to increase the risk of emergency ambulance dispatches for respiratory diseases at lag0 (per cent increase with a 10 μg/m3 increase=2.1%, 95% CI −2.1 to 6.3).6 In studies that used emergency department visits as a morbidity indicator, the point estimates for respiratory diseases were above unity, with or without statistical significance.25–30
In contrast with respiratory diseases, we did not observe any association between PM2.5 exposure and cardiovascular-related emergency ambulance dispatches, although PM2.5 exposure is strongly suspected to be a risk factor for cardiovascular diseases1: an increase risk of cardiovascular emergencies was shown in relation to PM2.5 exposure in Linz, Austria.6 However, not all studies report statistically significant associations between PM2.5 and cardiovascular disease-related mortality or morbidity probably because of demographic and geographic differences.31 ,32 The null association in our present study might be explained by difference in the pattern of cardiovascular diseases between Japan and Western countries: in Japan, the incidence of stroke is much higher than that of coronary heart disease,33 and while the association between PM2.5 and coronary heart disease has been documented, that between PM2.5 and stroke is still unclear.1 Further studies in terms of cardiovascular morbidity are required in Japan.
NO2 and SO2 exposure was positively associated in our study with emergency ambulance dispatches due to respiratory diseases. Observed associations were only for lag2–3, which might be explained by chance. However, exposure to NO2 and SO2 is known to be associated with respiratory symptoms,34 and NO2 exposure has the potential to adversely affect lung defence mechanisms against infection.35 In a recent panel study, short-term exposure to NO2 was linked with airway inflammation and/or oxidative stress in healthy and asthmatic adolescents aged 14–19 years.36 Exposure to SO2 is known to decrease lung function and increase airway resistance and respiratory symptoms.34 Since ambient SO2 contributes to acid aerosol formation, the health effects of acid aerosols are also pertinent.34 Although the biological mechanisms by which NO2 and SO2 exert adverse effects on the respiratory system are not fully understood, our findings are unsurprising.
One strength of our study is that the data included all emergency ambulance dispatches in Fukuoka City, so any selection bias caused by not covering all of the target subjects was negligible. In addition, we analysed approximately 176 000 cases, giving the study enough statistical power to detect even small effects of PM2.5 exposure and to estimate the precise effects of PM2.5 exposure on ambulance dispatch numbers. As a result, we were able to quantify the effect of PM2.5 exposure on ambulance dispatches regarding public health impact. The study also has some limitations, however. First, all data on PM2.5 concentrations came from a single monitoring station. While PM2.5 concentrations are known to be spatially homogeneous,37 exposure misclassification may have led to underestimation of the effects of PM2.5 on ambulance dispatches. Second, the cause-specific ambulance dispatches were classified on the basis of the initial diagnoses made by emergency physicians; these diagnoses might have changed later in some cases. However, a earlier study indicates no bias in the assignment of cardiopulmonary diagnoses related to daily air pollution concentrations in emergency departments.38 We think outcome misclassifications are likely to be non-differential, so we have no reason to suspect that using initial diagnoses affected the observed associations. Third, a possibility of residual confounding by influenza was left, because we did not obtain daily data on influenza incidence. A final limitation is that this study was performed in just one Japanese city, so further studies of other populations and locations are necessary to confirm the generalisability of our results.
In conclusion, by showing that exposure to PM2.5 was associated with emergency ambulance dispatches related to respiratory diseases, but not associated with cardiovascular-related dispatches, we have provided further evidence on the short-term health effects of PM2.5 exposure.
What is already known on this subject
-
There is growing evidence, particularly in Europe and the USA, of an association between short-term exposure to fine particulate matter (PM2.5) and mortality and morbidity.
What this study adds
-
We showed that exposure to PM2.5 was associated with an increased number of emergency ambulance dispatches (as a proxy of acute health outcomes) in Fukuoka City, western Japan.
-
To illustrate the public health impact, we estimated the extent to which a 10 μg/m3 decrease in PM2.5 concentrations would reduce the number of emergency ambulance dispatches.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors TM and KU specified the research question, and contributed to data collection, analysis, interpretation of results and drafting of the article. AT participated in analysis, interpretation of results and made critical revisions of the manuscript. MK and HH assisted with research design and contributed to data collection and critical revisions of the manuscript. TI assisted with research design, participated in interpretation of results and critical revisions of the manuscript. HN supervised the study and contributed to interpretation of results and critical revisions of the manuscript. All the authors approved the final version for submission.
-
Funding This study was supported by a Grant-in-Aid from the Ministry of Education, Culture, Sports, Science and Technology, Japan (25241015).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.