Article Text

Abstract
Background Previous studies have shown markedly lower birth weight among infants of South Asian origin compared with those of White European origin. Whether such differences mask greater adiposity in South Asian infants and whether they persist across generations in contemporary UK populations is unclear. Our aim was to compare birth weight, skinfold thickness and cord leptin between Pakistani and White British infants and to investigate the explanatory factors, including parental and grandparental birthplace.
Methods We examined the differences in birth weight and skinfold thickness between 4649 Pakistani and 4055 White British infants born at term in the same UK maternity unit and compared cord leptin in a subgroup of 775 Pakistani and 612 White British infants.
Results Pakistani infants were lighter (adjusted mean difference −234 g 95% CI −258 to −210) and were smaller in both subscapular and triceps skinfold measurements. The differences for subscapular and triceps skinfold thickness (mean z-score difference −0.27 95% CI −0.34 to −0.20 and −0.23 95% CI −0.30 to −0.16, respectively) were smaller than the difference in birth weight (mean z-score difference −0.52 95% CI −0.58 to −0.47) and attenuated to the null with adjustment for birth weight (0.03 95% CI −0.03 to 0.09 and −0.01 95% CI −0.08 to 0.05, respectively). Cord leptin concentration (indicator of fat mass) was similar in Pakistani and White British infants without adjustment for birth weight, but with adjustment became 30% higher (95% CI 17% to 44%) among Pakistani infants compared with White British infants. The magnitudes of difference did not differ by generation.
Conclusions Despite being markedly lighter, Pakistani infants had similar skinfold thicknesses and greater total fat mass, as indicated by cord leptin, for a given birth weight than White British infants. Any efforts to reduce ethnic inequalities in birth weight need to consider differences in adiposity and the possibility that increasing birth weight in South Asian infants might inadvertently worsen health by increasing relative adiposity.
- BIRTH WEIGHT
- EPIDEMIOLOGY
- ETHNICITY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Infants born in South Asia tend to have lower mean birth weights than infants born elsewhere in the world, including those born in other low-income countries.1 This is, in part, thought to reflect poor maternal nutrition throughout their life course, including during pregnancy. However, infants born in high-income countries, such as the UK and the USA to mothers of South Asian origin, are also considerably lighter than babies born to white mothers2 ,3 Lower birth weight is related to adverse perinatal outcomes4 ,5 and has also been associated with a number of common chronic diseases of adulthood, including cardiovascular disease and type 2 diabetes.6–8 It has therefore been suggested that the risk factors for lower birth weight among South Asian infants should be identified and interventions aimed at increasing their birth weight be developed.3 ,9 However, there is some evidence that, relative to their lower birth weight, South Asian infants are more adipose at birth than European infants (ie, that for a given birth weight they carry relatively more fat mass).10–13 This would be consistent with findings in infants (6–12 weeks), children and adults suggesting that for a given body mass those of South Asian origin have more total fat and are more prone to centrally distributed fat than European origin adults and children.14–17
If South Asian-origin infants do have more fat at birth than European infants, then any public health interventions to increase their birth weight could inadvertently increase fat mass and potentially worsen their later cardiometabolic health, thus increasing the already existent ethnic inequalities in diabetes and coronary heart disease.18 Evidence to date for the existence of such differences at birth is scant. To our knowledge, only four previous studies have compared markers of fat mass or distribution between South Asian and White European origin infants at birth. All suggested that South Asian infants tended to have greater central adiposity and fat mass for a given weight than the European infants.10–13 However, these studies had relatively small sample sizes (224, 969, 1040 and 560, respectively) and three of them compared South Asian infants born in India to European infants born in the UK or the Netherlands.10–13 It is possible that the differences in these studies reflect geographical-related rather than ethnic-related mechanisms. To our knowledge, just one small study has compared the UK-born South Asian-origin infants (N=165) and British infants (N=343).13
One method that has been used to try and understand mechanisms underlying birth weight differences has been to look across generations. The assumption here is that if poor maternal nutrition is an important determinant of the birth weight differences, then when mothers (as well as infants) have been born in a more affluent country and potentially exposed to better nutrition, the difference should be smaller. Furthermore, the narrowing of the difference would be expected to increase across generations as populations become more assimilated and intergenerational effects on poor growth are less prominent, though we acknowledge that some immigrant populations may not assimilate and may maintain similar diets to those prior to immigration. Of the five previous studies that have looked at birth weight differences in the UK between European and South Asian origin infants across generations,3 ,9 ,19–21 four found no clear evidence of a narrowing of the difference with subsequent generations,3 ,9 ,19 ,20 and one small study (N=331) found some increase in birth weight in second generation compared with the first.21 In most of these studies, generation has been defined according to maternal place of birth. This approach assumes that paternal place of birth does not contribute to the ethnic differences in birth weight, but both paternal and maternal birth weight and adult height are associated with offspring birth weight22 and it is possible that both mothers’ and fathers’ nutritional status and other environmental exposures could influence the offspring's birth size. Fathers could influence infant birth weight indirectly via fathers influencing their partners diet and hence pregnancy nutritional status (ie, if fathers are UK born, the mother may be more or less likely to have changed her diet to that of the UK population than if the father is not UK born). It has also been suggested that fathers can influence offspring growth via parent of origin/epigenetic effects,23, though we are as yet unaware of any direct evidence to support this. To our knowledge, no previous study has compared differences in indicators of birth fatness (skinfolds and cord leptin) between different generations of the UK born South Asian infants.
The aim of this study was to compare the birth weight, skinfold thickness and cord leptin between Pakistani and White British infants and to investigate explanatory factors, including the place of birth of parents and grandparents. The skinfold thicknesses are used as indicators of fatness24 with subscapular skinfolds indicating centrally distributed fat25 and allow comparisons with previous studies that have also used skinfold measurements to compare adiposity between South Asian and European origin infants.10–13 In addition, we have compared cord leptin, which provides a more accurate reflection of total infant fat mass26 between the two groups.
Methods
Participants
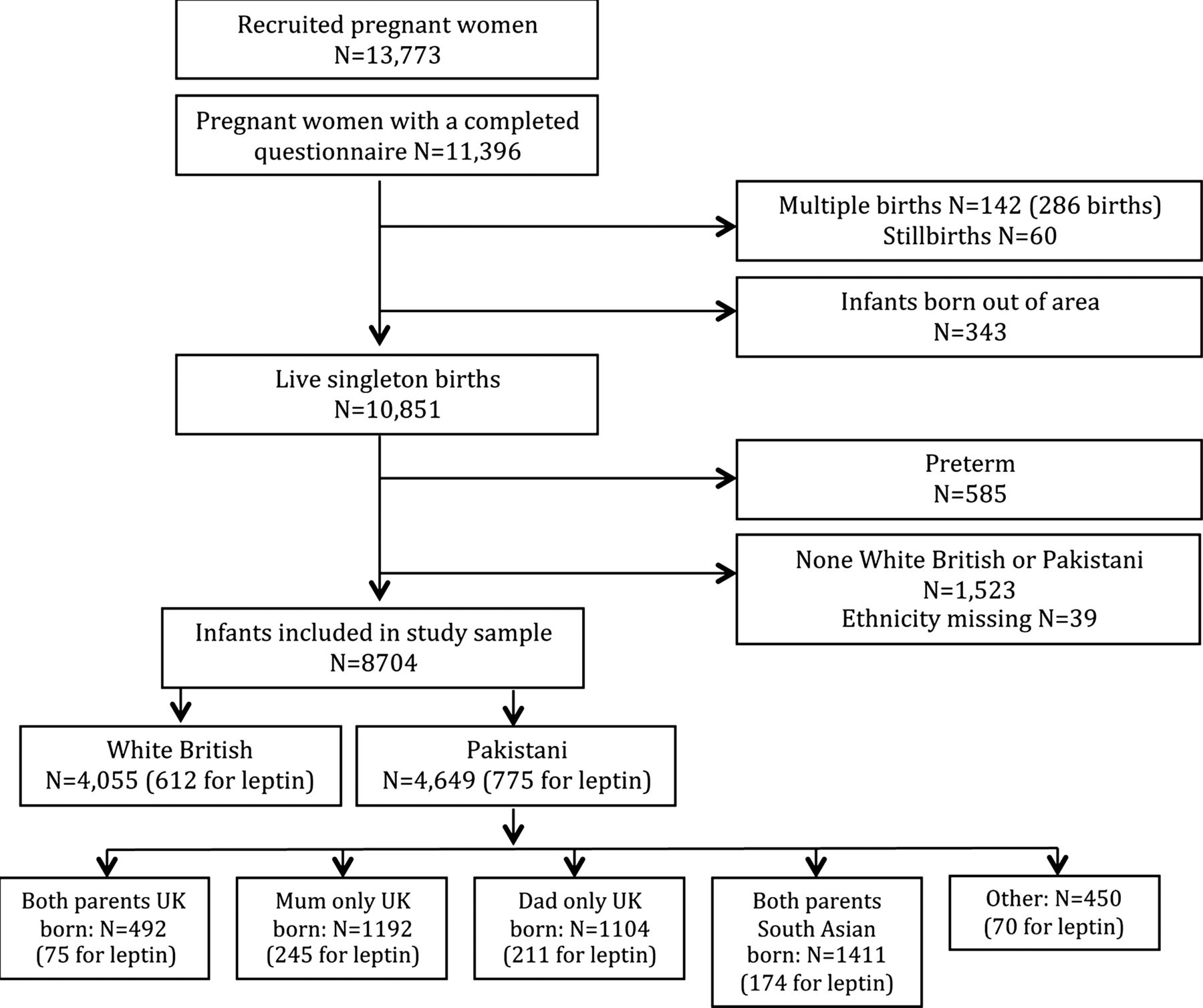
The Born in Bradford (BiB) study is a prospective birth cohort study that recruited women during pregnancy and has followed them, their infants and their partners into the child's infancy. To be eligible for the study, women had to attend booking clinic between March 2007 and December 2010 and be booked to give birth in Bradford. Full details of the study methodology have been previously reported.27 Women were recruited at their oral glucose tolerance test (OGTT) appointment; all women booked for delivery in Bradford are offered a 75 g OGTT at around 26–28 weeks gestation. Women who attended this appointment completed an interviewer-administered questionnaire and had their height and weight measured. Interviews were conducted in a range of South Asian languages (including Mirpuri, Bengali, Punjabi). For these analyses, infants born at less than 37 weeks gestation, stillbirths, multiple births and infants born to parents of ethnic origin other than White British or Pakistani were all excluded (figure 1). Thus, 8704 participants are included (4649 Pakistani and 4055 White British).

Study sample.
Outcome measurement
Birth weight was abstracted from the medical records and in all participants was recorded immediately following birth. Subscapular and triceps skinfold measurements were collected by trained research administrators and most were measured within the first 24 h following birth and all within 72 h.28 Measurements were obtained using Harpenden Calipers (Holtain Ltd) on the left side of the body. We have previously shown good levels of within and between assessor reliability for all the birth size measurements.25 Cord blood samples were obtained at delivery by the attending midwife on a consecutive subsample (n=1387). Samples were refrigerated at 4°C in EDTA tubes until collected by laboratory staff within 12 h. Samples were spun, frozen and stored at −80°C. Once all samples had been collected, they were transferred to the Biochemistry Department of Glasgow Royal Infirmary for analysis. Leptin was measured by a highly sensitive in-house ELISA with better sensitivity at lower levels than commercial assays as previously described.29
Exposure measurement
Ethnicity was self-reported at interview, with participants given response options based on the UK Office of National Statistics guidance.30 Pakistani-origin women completed a detailed ancestry interview which included the details of the place of birth of themselves, their partner and all four grandparents. Generational status of Pakistani infants was based on these data. Using information on both parents and all four grandparents produced 66 possible unique categories. We examined the numbers, mean birth weight and SD in all categories and then combined the groups based on sample size and similarities in mean birth weight and migration history. This resulted in 17 categories within which 90% fell into one of the four main categories:
Both parents UK born and all grandparents South Asian born
Mother UK born, father and all grandparents South Asian born
Father UK born, mother and all grandparents South Asian born
Both parents South Asian born and all grandparents South Asian born
The remaining 10% fell across the other 13 categories, each of which included relatively few participants and so these groups were combined to form one ‘other’ category. As all grandparents were South Asian born (with the exception of the ‘other’ group), and to simplify interpretation, the generation groups were labelled according to the place of birth of parents only for the remainder of the paper.
Covariables
Few characteristics could plausibly influence a woman's ethnicity and therefore confound the association of this with outcomes.31 ,32 However, we were interested in characteristics that are known to be influenced by ethnicity and that might be on a causal pathway explaining birth size differences. In addition, we were aware that some characteristics might mask differences. For example, women of White British origin are more likely to smoke during pregnancy than those of Pakistani origin and taking account of this may in fact increase the ethnic difference in birth weight. While such characteristics cannot be on a mediating causal pathway (since accounting for their ethnic differences would likely increase rather than decrease birth weight differences), we felt it important to explore the effect of adjusting for them on ethnic differences in birth size. A priori, we considered maternal early pregnancy body mass index (BMI), height, age, parity, smoking, alcohol consumption, socioeconomic position (maternal education, housing tenure, whether they received benefits), living with a partner, fasting and postload glucose, fasting insulin, hypertensive disorders of pregnancy, infant sex and gestational age to be characteristics that might explain or mask ethnic differences in outcomes. Online supplementary table S1 briefly summarises our a priori assumptions of directions of association between ethnicity and each of the characteristics and between each of these and birth weight and hence the potential impact that they might have on birth weight differences between Pakistani and White British infants. Maternal weight (SECA digital scales) and height (Leicester Height Measure) were measured in light clothing and unshod.27 Fasting and postload glucose and fasting insulin were obtained from the OGTT samples which were assayed immediately after sampling at the biochemistry department of Bradford Royal Infirmary using the glucose oxidase method on Siemen's Advia 2400 chemistry autoanalysers and Siemen's Advia Centaur assay. Information for all other covariables was obtained from medical records or the mother's questionnaire.27
Statistical analysis
All analyses were performed using STATA (V.11). Multivariable linear regression was used to examine the associations between ethnicity and birth weight, skinfolds and cord leptin levels (Pakistani infants compared with White British infants) and to examine these associations by generation (each Pakistani generation group compared with White British infants). We adjusted separately for each covariable to see how these influenced the associations and then adjusted (1) jointly for those that we thought a priori (see online supplementary table S1) would plausibly be on the causal pathway for lower birth size in Pakistani origin infants; (2) jointly for those that did reduce the difference when adjusted for individually; and (3) for all covariables simultaneously. We generated sex and gestational age internal standardised z-scores for birth weight and skinfold thicknesses using six gestational age categories (37; 38; 39; 40; 41; 42–42) so that these were all assessed on the same scale and could be directly compared. We then regressed these scores on ethnicity to calculate the mean difference in z-score between White British and Pakistani infants. Further, we adjusted for birth weight in the regression analyses of skinfolds (z-scores) and cord leptin. Cord leptin concentration had a positively skewed distribution and was natural log transformed to achieve approximate normality of the residuals in the regression models. The resultant coefficients were back transformed to give ratios of geometric means which have a null value of 1. Owing to the smaller leptin sample size, we only included covariables in the final model that altered the coefficient when each was examined individually.
Missing data
For the main analyses, we included only participants with complete data on exposure, each outcome and all covariables. This resulted in 8704 participants for birth weight analyses; 6041 for subscapular skinfolds; 6058 for triceps skinfolds; and 1186 for cord leptin analyses. In order to examine whether missing covariable data might have biased our results, we repeated unadjusted analyses and analyses adjusting just for one covariable (taking each in turn) in maximal samples (ie, not restricting to those with complete data on all covariables) and compared results with the equivalent results in those with complete data on all covariables (see online supplementary tables S3–S6).
Results
Pakistani-origin mothers were on average older, shorter and had a lower BMI than White British origin mothers (see online supplementary table S2). They were more likely to be married, but less likely to be employed. Few Pakistani mothers reported smoking during pregnancy and none reported having consumed alcohol while pregnant. There were fewer UK-born Pakistani mothers in this sample than South Asian born and the largest Pakistani generation group was that where both parents were born in South Asia. Some characteristics varied across generation groups according to the maternal birthplace including employment and smoking during pregnancy which were both more common among UK-born Pakistani mothers. Other characteristics differed by the partner's place of birth irrespective of whether the mother was UK or South Asian born, including maternal BMI which was higher among Pakistani mothers with a South Asian-born partner compared with those with a UK-born partner.
Birth weight was lower among Pakistani infants than White British infants (figure 2 and see online supplementary table S3; unadjusted mean difference −235 95% CI −256 to −214). Maternal height, maternal BMI and gestational age all explained some of the differences, but important differences remained even with adjustment simultaneously for these three characteristics (see online supplementary table S3). Smoking, maternal fasting glucose, parity and living with a partner all masked some of the difference. The combined effect of adjusting for all covariables simultaneously was that the mean birth weight difference was similar to the unadjusted difference (figure 2 and see online supplementary table S3). Across generation groups, the adjusted mean difference in birth weight was least where both parents were UK born (−217 95% CI −261 to −173) and greatest when just the mother was UK born (−253 95% CI −285 to −222), but there was no strong statistical evidence that the association of ethnicity with birth weight varied by generational group (all p values ≥0.1).
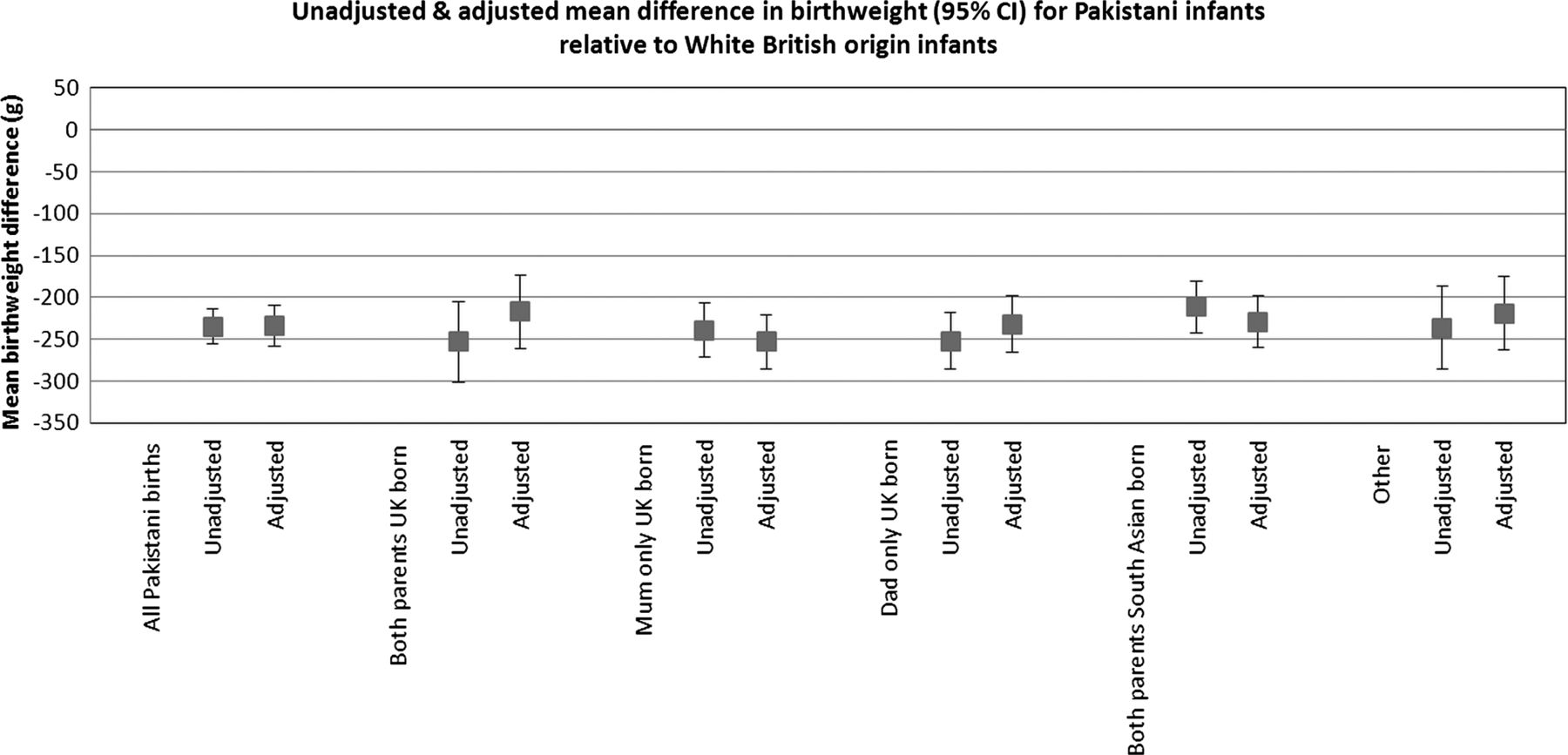
Unadjusted and adjusteda mean difference in birth weight (95% CI) between Pakistani and White British infants. aAdjusted for smoking; alcohol; maternal age; maternal hypertension; maternal fasting glucose; maternal height; maternal body mass index; parity; gestation; sex; socioeconomic position (maternal education, housing tenure, receipt of means tested benefits); and living with partner. Fasting glucose, postload glucose and fasting insulin were highly correlated thus postload glucose and fasting insulin were excluded from the fully adjusted model as they had the least effect and no impact on associations over that seen for fasting glucose. This figure is only reproduced in colour in the online version.
Subscapular and triceps skinfold thickness were each smaller among Pakistani infants compared with White British infants (figures 3 and 4, see online supplementary tables S4 and S5). The adjusted mean difference in subscapular and triceps skinfold was greatest when mothers were South Asian born and fathers were UK born (−0.36 95% CI −0.47 to −0.26 and −0.32 95% CI −0.42 to −0.21, respectively) and least for subscapular skinfold when both parents were UK born (−0.22 95% CI −0.36 to −0.08) and for triceps skinfold where mothers were UK born and fathers South Asian born (−0.22 95% CI −0.32 to −0.12). As with birth weight, differences between groups were generally small and again there was no strong statistical evidence of differences between generational groups (all p values ≥0.1 and 0.3, respectively, for subscapular and triceps differences).

Unadjusted and adjusteda mean difference in subscapular skinfold between Pakistani and White British infants. aAdjusted for smoking; alcohol; maternal age; maternal hypertension; maternal fasting glucose; maternal height; maternal body mass index; parity; gestation; sex; socioeconomic position (maternal education, housing tenure, receipt of means tested benefits); and living with partner. Fasting glucose, postload glucose and fasting insulin were highly correlated thus postload glucose and fasting insulin were excluded from the fully adjusted model as they had the least effect and no impact on associations over that seen for fasting glucose. This figure is only reproduced in colour in the online version.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Unadjusted and adjusteda mean difference in triceps skinfold between Pakistani and White British infants. aAdjusted for smoking; alcohol; maternal age; maternal hypertension; maternal fasting glucose; maternal height; maternal body mass index; parity; gestation; sex; socioeconomic position (maternal education, housing tenure, receipt of means tested benefits); and living with partner. Fasting glucose, postload glucose and fasting insulin were highly correlated thus postload glucose and fasting insulin were excluded from the fully adjusted model as they had the least effect and no impact on associations over that seen for fasting glucose. This figure is only reproduced in colour in the online version.
Mean z-score differences were lower for subscapular and triceps skinfold thickness than birth weight (table 1); once the differences in birth weight were adjusted for, the z-score differences in skinfold thickness were markedly reduced or became weakly positive (table 2). Cord blood leptin levels were similar among Pakistani and White British infants without the adjustment for birth weight (table 3); but, with adjustment for birth weight, Pakistani infants had a cord leptin value on average 30% higher (ratio of geometric means 1.30 95% CI 1.17 to 1.44) than White British infants. Differences did not differ markedly across generation groups.
Adjusted mean z-score differences in Pakistani relative to White British infants
Adjusted mean z-score differences in Pakistani relative to White British infants with adjustment for birth weight
Adjusted differences in cord leptin between Pakistani and White British infants
Discussion
Main findings
These results suggest a striking difference in birth weight between Pakistani and White British infants which persists even after the adjustment for a wide range of potential mediating characteristics and is maintained over successive generations. We found evidence of greater relative adiposity in Pakistani infants compared with those of White British origin. Notably, once birth weight had been taken into account, cord leptin, used as a marker of total fat mass, was higher in Pakistani origin compared with White British-origin infants suggesting that infants of Pakistani origin are lighter, but relatively fatter, than those of White British origin. This is by far the largest study to date to examine these associations and highlights the importance of considering body composition, and not just weight, when considering ethnic differences in birth size.
Our finding that birth weight differences between Pakistani and White British origin infants do not vary notably by Pakistani generation is consistent with most previous studies9 ,19 ,20 However, we have added to this previous literature by showing that this is also the case when generation is defined by paternal (and not only maternal) place of birth.
We found marked differences in pregnancy, behaviour and socioeconomic characteristics between Pakistani and White British mothers that had varying effects on the associations between ethnicity, generation and birth size. Smoking, maternal fasting glucose, parity and living with a partner all masked some of the differences, and also gestational length, maternal height and BMI individually explained some. From these results, there is no clear way in which the ethnic differences in birth size could be reduced. Levels of smoking are modifiable, but reducing smoking in White British women, while desirable, would only increase ethnic differences. Effective treatment of hyperglycaemia in pregnant women would be beneficial, but based on our results would likely increase ethnic differences in birth weight, although given the relationship of greater maternal glycaemia with greater adiposity (see online supplementary table S6), could reduce the greater relative adiposity in Pakistani-origin infants. Characteristics such as parity, marital status, gestational length and maternal height are not clearly modifiable during pregnancy. Finally, interventions to increase BMI in Pakistani mothers would potentially be disadvantageous for both the mother's and her offspring's health, as they would increase the mother's risk of gestational diabetes and later adverse cardiometabolic health and potentially the risk of greater relative adiposity in offspring.
Comparison with other studies
Our findings add importantly to the four previous studies10–13 exploring whether the ethnic difference in relative body fat found in studies comparing South Asian and White European origin adults and schoolchildren,14 ,15 is present at birth. Our study is considerably larger than these previous studies and compares Pakistani infants to White British infants who were all born in the same UK maternity unit, and thus controls for the possible differences that may occur between births in a South Asian country and those in the UK.
While generally consistent with previous studies, we found no clear evidence of greater relative central adiposity in Pakistani infants compared with White British infants which some previous studies have reported based largely on comparing subscapular to triceps differences between ethnic groups.10–13 These studies have been smaller than ours and largely compared South Asian-born infants to UK-born European infants, and it is possible that central adiposity is greater in South Asian infants born in South Asia, but not in those born in the UK. This has some support from a study of UK schoolchildren which found, consistent with our results, greater markers of general adiposity, but a lower waist circumference in UK South Asian compared with White European children.33
Study strengths and limitations
The key strengths of this study are its large sample size, detailed information on place of birth of mothers, fathers and all four grandparents, the ability to adjust for a much wider range of possible explanatory or masking variables than any previous study and the availability of cord leptin to assess relative differences in fat mass. Limitations include some missing covariable data. However, patterns of missing data were similar by ethnic group and unadjusted associations in each group did not differ markedly between those with some data and those with complete data on all covariables. It is possible that BMI is a less accurate measure of adiposity among South Asian mothers than White British mothers; however, the plausible mechanism by which maternal BMI might influence offspring fatness would be via glucose intolerance, and here we have used a gold standard (OGTT) measure of this and have shown that adjustment for fasting glucose, postload glucose or fasting insulin do not substantively explain the ethnic differences reported here. Cord leptin measurements were only available for a subgroup, but these were a consecutive sample and we can see no reason why collecting these over a specific time period would result in a select group; similar proportions from each ethnic group had cord leptin data. We had hoped to be able to explore the generational effects across a larger range of generational groups, but for the vast majority of participants in the study all four grandparents were born in South Asia and so we were unable to examine whether place of birth of grandparents influenced the differences. Nonetheless, this pattern of migration to Bradford is in itself interesting and relevant to future health needs in the city. While our findings for birth weight are largely consistent with a number of other studies that have explored broader South Asian groups and/or looked at different groups (eg, Pakistani, Indian and Bangladeshi origin) and found in general all have lower birth weight than White British infants,3 ,9 ,13 ,19 ,20 we cannot be certain that the results are generalisable to other South Asian groups. There are participants of Indian and Bangladeshi origin in BiB, but the numbers were too small for meaningful analyses, particularly across generations or for cord leptin concentration, therefore they were excluded from this paper.
Conclusion
To conclude, our results suggest that despite being markedly lighter, Pakistani infants have greater fat mass (as assessed by cord leptin) for a given birth weight than White British-origin infants. Further studies are needed to explore whether efforts to increase birth weight in Pakistani infants and hence to reduce the ethnic difference could inadvertently result in even greater relative adiposity which in turn may worsen long-term health outcomes for Pakistani infants.
What is already known on this subject
-
Infants born in South Asia are on average smaller and lighter at birth than infants born elsewhere in the world, and this difference persists among the South Asian-origin infants born in high-income countries including the UK.
-
Previous studies have found no clear evidence that mean birth weight is increasing in subsequent generations of the UK South Asians.
-
South Asian children and adults have greater fat mass for a given weight or body mass index, but whether this is the case at birth is unclear.
What this study adds
-
For a given birth weight, Pakistani-origin infants have greater adiposity than White British-origin infants born at the same UK maternity hospital.
-
Ethnic differences in adiposity do not vary notably depending on whether both mothers and fathers of Pakistani-origin infants are born in the UK or South Asia.
-
Efforts to increase birth weight in South Asian-origin infants could inadvertently result in even greater relative adiposity.
Acknowledgments
The authors would like to thank all the paediatricians, obstetricians and midwives involved in training, recruitment and data collection for the BiB study. We also thank the BiB study administrators and study team. We are especially grateful to all the mums, dads and babies who are taking part in BiB. We also thank Professor Dave Leon for his advice and comments during the development of this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors JWe, DAL and JWr conceived the study idea and developed the analysis plan; JWr is overall PI for BiB and directed data collection, with input from JWe, DAL, RB, NC and PAM; JWe undertook the main analysis with input from LF and supervision from DAL and JWr; NS secured funding for and completed cord leptin assays; JWe, DAL and JWr wrote earlier versions of the paper and all authors contributed to critical review and the final version.
-
Funding Cord leptin assays were funded by a British Heart Foundation Project Grant (PG/09/036/27380). JWe is funded by a UK Medical Research Council (MRC) Special Training Fellowship in Health of the Public and Health Services Research (MRCGO601712), DAL works in a centre that receives funding from the MRC (G0600705).
-
Competing interests None.
-
Ethics approval Ethics approval for the study was provided by Bradford Local Research Ethics Committee (ref 06/Q1202/48).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Scientists are encouraged and able to use BiB data. Data requests are made to the BiB executive using the form available from the study website http://www.borninbradford.nhs.uk (please click on ‘Science and Research’ to access the form). Guidance for researchers and collaborators, the study protocol and the data collection schedule are all available via the website. All requests are carefully considered and accepted where possible.