Article Text

Abstract
Background Research has linked food insecurity to mental health problems, though little is known about this relationship among Canadian youth. We investigate the association between food insecurity severity and mental illnesses in a nationally representative youth sample.
Methods We sampled 55 700 youth 12–24 years from recent cycles of Canadian Community Health Survey. Household food insecurity was measured using a standard 18-item questionnaire. We fitted Poisson regressions on self-rated mental health and diagnosed mood and anxiety disorders, controlling for sociodemographic confounders. Clinical assessments of emotional distress, major depression and suicidal ideation were examined in subsamples with available data. We stratified the sample by gender, age and survey cycle to test potential demographic heterogeneity.
Results One in seven youth lived in marginal (5.30%), moderate (8.08%) or severe (1.44%) food insecurity. Results showed that food insecurity was associated with higher likelihood of every mental health problem examined. The association was graded, with more severe food insecurity linked to progressively worse mental health. Notably, marginal, moderate and severe food insecurity were associated with 1.77, 2.44 and 6.49 times higher risk of suicidal thoughts, respectively. The corresponding relative risk for mood disorders were 1.57, 2.00 and 2.89; those for anxiety disorders were 1.41, 1.65 and 2.58. Moderate food insecurity was more closely associated with mental health problems in 18–24 year olds than in 12–17 year olds.
Conclusions Food insecurity severity was associated with poorer mental health among Canadian youth independent of household income and other socioeconomic differences. Targeted policy intervention alleviating food insecurity may improve youth mental health.
- mental health
- suicide
- depression
- adolescents
- health inequalities
Data availability statement
Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are accessible through Statistics Canada with restrictions. For the present study, the data were accessed under contract through the Statistics Canada Research Data Centre at the University of Toronto.
Statistics from Altmetric.com
Food insecurity, defined as the inadequate access to food due to financial struggles, is a public health challenge that affects one in eight households in Canada,1 including disproportionate shares of underage children and young adults.1 2 Food insecurity constitutes a significant risk factor for mental illnesses,3 4 which affects one-quarter of Canadian youth aged 9–19 years.5 Many mental health problems in youth track strongly into adulthood, culminating in more serious illnesses.6 Prevention and treatment at early ages are necessary and cost-effective.7
Food insecurity tends to co-occur with poverty and socioeconomic adversities in general, which jeopardise mental health management by reducing access to medications and non-urgent psychotherapy.8 9 Poor access to food may also result in nutrient inadequacy and poor diet,10 which affect brain development and mental health through gut microbiota and other mechanisms.11 Moreover, food insecurity is a visceral reminder of social disadvantage. The inability to afford food and stigma attached to accepting food charity elicits stress, shame and anxiety,12 which may elicit or exacerbate mental disorders via chronic hypothalamic–pituitary–adrenal activation.13
Limited evidence links food insecurity to youth mental health, particularly in Canada.14–16 Previous studies that included children or youth have either narrowly assessed hunger (an extreme form of food insecurity),14 15 were limited to a single province16 or failed to adjust for socioeconomic confounders.16 Some research associated food insecurity with youth mental health in the USA and globally17–25; however, only one study accounted for severity of food insecurity17 while none evaluated demographic heterogeneity within youth.
We drew on recent community health surveys in Canada to investigate the association between food insecurity severity and mental illness in nationally representative samples of youth. We used multiple indicators of mental illness and stratified the analyses by age, gender and cohort. Our goal was to provide contemporary evidence on the strength and consistency of this association across groups and domains of mental health.
Methods
Study design and population
This study used three recent cycles of the Canadian Community Health Survey (CCHS; 2007–2008, 2011–2012 and 2017–2018). CCHS is a biennial cross-sectional survey representing 98% of the Canadian non-institutionalised population 12 years or older. The CCHS randomly samples households nationwide based on geographic areas, telephone numbers and Canadian Child Benefit frames while weighting on respondent’s location, gender and age.26 The survey interviews approximately 130 000 households by phone or in person per 2 year cycle and includes a standardised measurement of household food security. The three cycles we chose are the only cycles with nationally representative data on food insecurity. One member per household is randomly selected to answer questions about themselves and on behalf of the household. Formal consent must be first obtained from parents or adult guardians before interviewing a selected adolescent below age 16. Food insecurity and income questions are answered by an adult household member when the selected interviewee is below age 18 (or below 16 in 2007–08).
There were 57 800 respondents aged 12–24 in the three CCHS cycles (online supplemental eFigure 1). We excluded cases with missing food insecurity status and children living without an adult. The analytic sample comprised 55 700 youth with valid household food insecurity status. We used this sample to study outcomes measured nationwide consistently over time, including self-rated mental health status and clinically diagnosed mood disorders and anxiety disorders. We also analysed subsamples with valid responses to questions on emotional distress (n=12 400), major depression (n=10 800) and suicidal ideation (n=40 000); this was optional survey content selected by some provinces and territories (online supplemental etable 1).
Supplemental material
Measures
All six outcomes were dichotomised. The three outcomes measured consistently in all jurisdictions were concurrent self-rated mental health status (fair or poor vs excellent, very good or good), previously diagnosed mood disorders (depression, bipolar disorder, mania or dysthymia) and anxiety disorders (phobia, obsessive–compulsive disorder or panic disorder). The prevalence of mood and anxiety disorders reported by youth was similar to that from administrative records.27 The three outcomes with optional jurisdiction-cycle participation were past month emotional distress measured by Kessler Psychological Distress Scale (K-10)28 ; past year major depression measured by WHO’s Composite International Diagnostic Interview-Short Form (CIDI-SF) for major depression29 ; and past year suicidal ideation (see online supplemental eTable 2 for operationalisation of the outcomes). Depression and suicidal ideation were not measured in the 2017–2018 cycle. Questions were administered directly to respondents of all ages.
The exposure of interest was household food insecurity status, a four-category variable derived from 18 survey questions on a household’s access to food over the past 12 months. The questions cover food hardships, ranging from the less serious and more common ‘worries about food running out’ to more damaging and less common ‘not eating for a whole day’.30 Negative answers to all questions would categorise a household as food-secure, whereas having any affirmative answer would make a household marginally, moderately or severely food-insecure, depending on the number of affirmations (online supplemental eTable 3). The food security questionnaire was created and validated by US Department of Agriculture and later adapted for the CCHS by Health Canada.30
We adjusted for potential confounders in associations between food insecurity and mental illness.4 They included individual demographic characteristics (gender (male/female), age (in years) and race–ethnicity (white/Black/Indigenous/others)), household socioeconomic characteristics (highest education in household, household income, housing tenure and household type), province or territory of residence and survey cycle. Statistics Canada imputed missing household income for approximately one-quarter of the sample, which we controlled for using a dummy variable. Missing values from other categorical covariates were negligible and denoted in a separate category in their respective variable.
Statistical analysis
We used Poisson regressions with robust variance estimators to estimate adjusted risk ratios (aRRs) of mental health outcomes in relation to household food insecurity, controlling for the aforementioned covariates. Because mental disorders are more prevalent among young adults than adolescents,5 we examined the potential interaction effect of age on the association between food insecurity and the nationally measured mental health outcomes. Given a greater susceptibility to mental disorders in females than males,6 we also examined the moderating effect of gender for these outcomes. Since mental health issues have become increasingly prevalent over time,5 we further examined the interaction between food insecurity and the three CCHS cycles. We did not test interactions with age, gender or CCHS cycle on the three outcomes from the optional survey content due to smaller sample sizes. For sensitivity analyses, we experimented with excluding the northern territory of Nunavut, which was considered an outlier jurisdiction due to its extremely high food insecurity prevalence.1 For distress and depression, we tested different cut-off thresholds and linear models on log forms of the outcomes. We used Stata SE V.15.1 to estimate two-sided confidence intervals, setting the significance threshold to p<0.05. Multivariate analyses were unweighted; person weights were used in descriptive analyses to calculate population means. Average predicted probabilities were estimated on the fully adjusted models using the sample and subsamples. Number of observations were rounded to protect identity. This study was approved by the Health Sciences Research Ethics Board at University of Toronto.
Results
Of the 55 700 sampled youth, there were 5.30% (2950), 8.08% (4500) and 1.44% (800) individuals from marginally, moderately and severely food-insecure households (table 1). Compared with those from food-secure households, youth in food-insecure households were more likely to report fair or poor mental health, mood disorders, anxiety disorders and emotional distress. Major depression and suicidal ideation were more prevalent among youth from moderately or severely food-insecure households than among their food-secure counterparts. Income was substantially lower for food-insecure households than for food-secure ones. Other socioeconomic disadvantages such as incomplete high school education also grew more prevalent as food insecurity worsened.
Sample characteristics by food insecurity status based on CCHS 2007–2008, 2011–2012 and 2017–2018
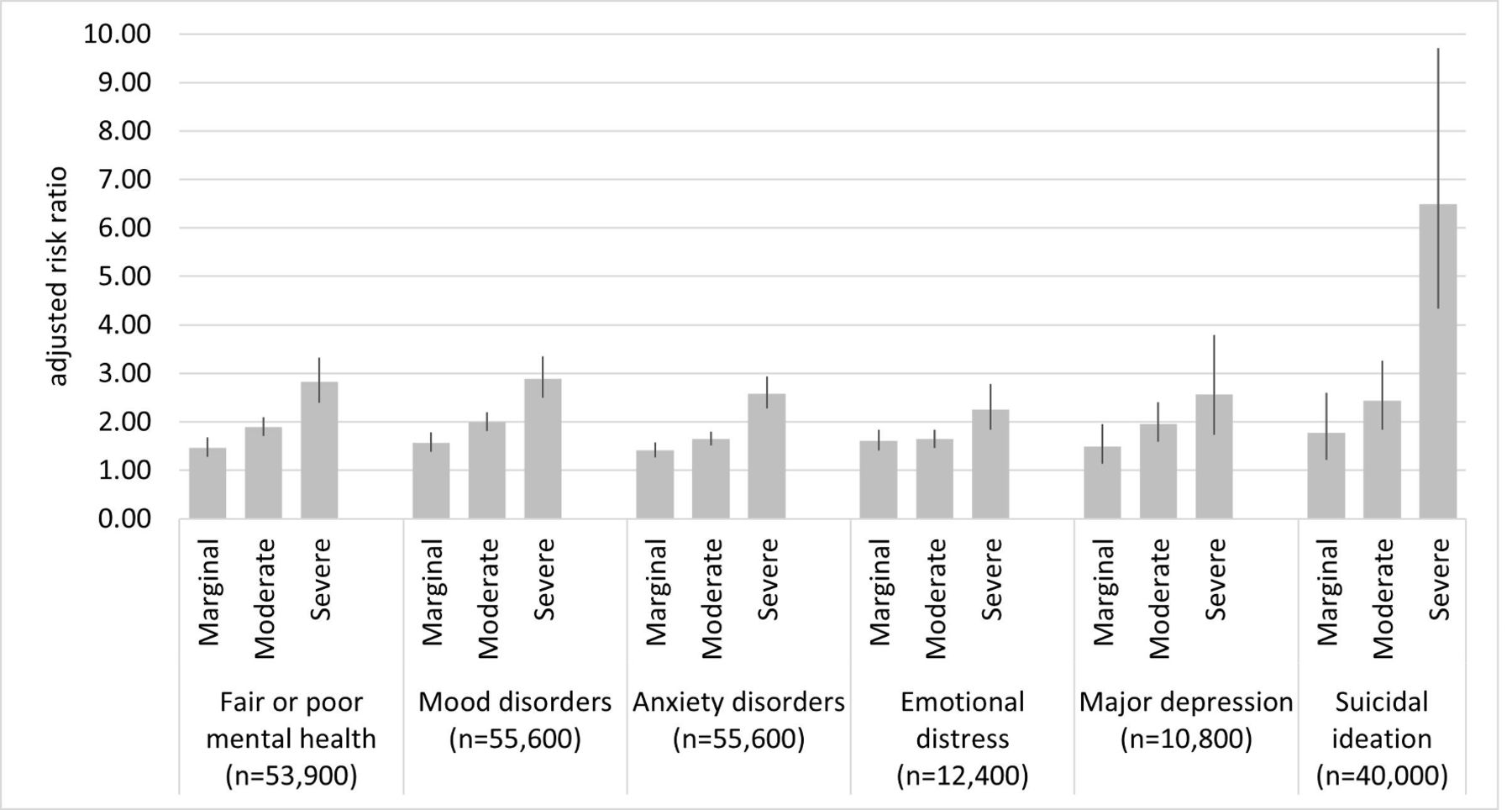
The severity of food insecurity shared a graded association with all mental health outcomes after adjusting for sociodemographic differences (figure 1; online supplemental eTable 4). Compared with food-secure youth, those in marginal, moderate and severe food insecurity were 1.46, 1.89 and 2.82 times more likely to report fair or poor mental health status, respectively. Marginal, moderate and severe food insecurity was associated with 1.57, 2.00 and 2.89 times higher risk of mood disorders, respectively. The corresponding aRR for anxiety disorders were 1.41, 1.65 and 2.58, respectively.
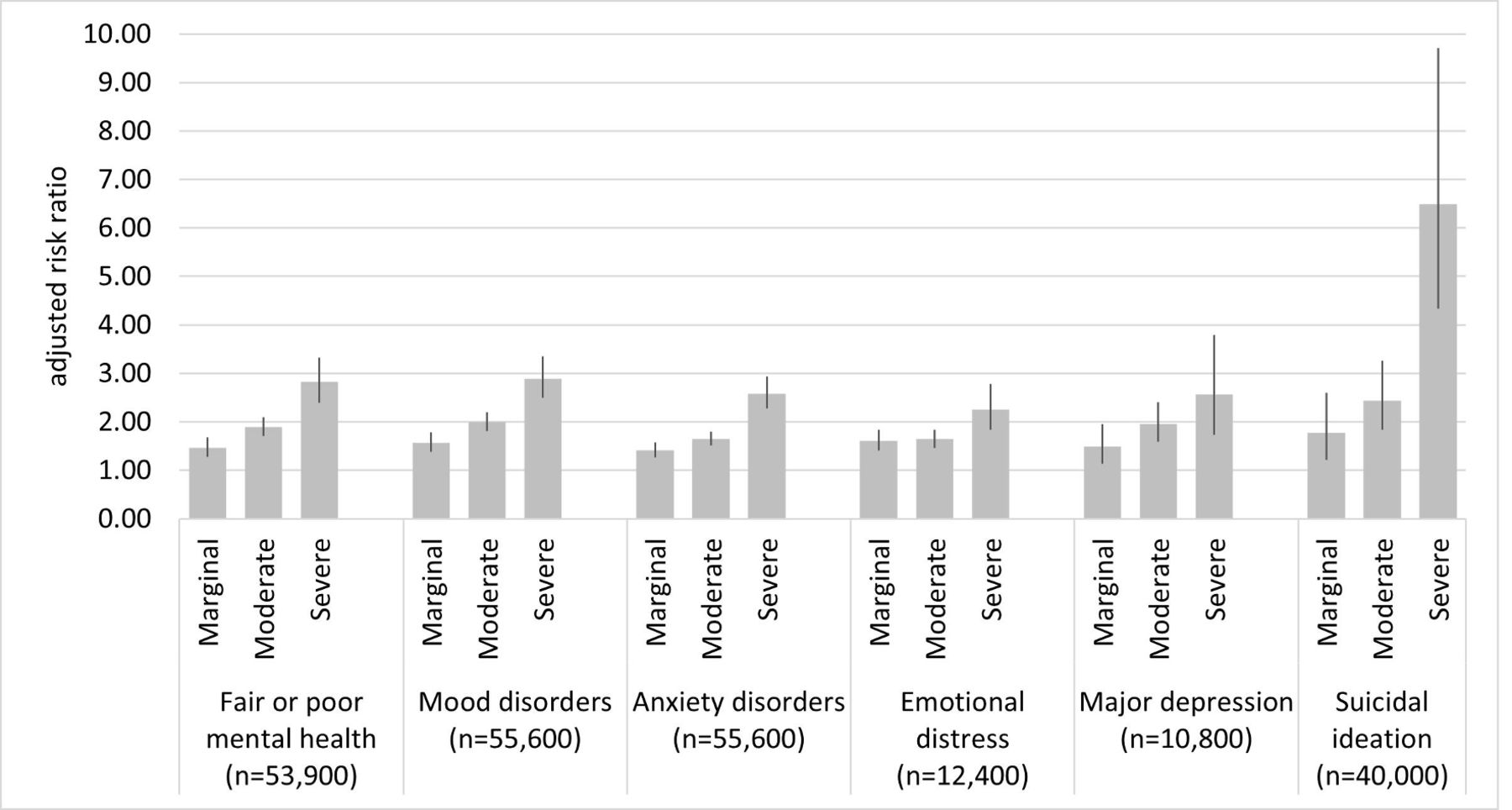
Poorer mental health associated with food insecurity among youth 12–24 years old. Data show risk ratios of marginal, moderate and severe food insecurity on six binary outcomes of mental health problems among overall youth 12–24 years old, adjusting for socioeconomic confounders. Reference group is food-secure youth.
For the three optional outcomes, marginal, moderate and severe food insecurity were associated with 1.61, 1.64 and 2.26 times greater risk of experiencing emotional distress, respectively. Marginal, moderate and severe food insecurity also corresponded to 1.49, 1.96 and 2.56 times greater risk of major depression and 1.77, 2.44, and 6.49 times greater risk of suicidal ideation in the past year, respectively.
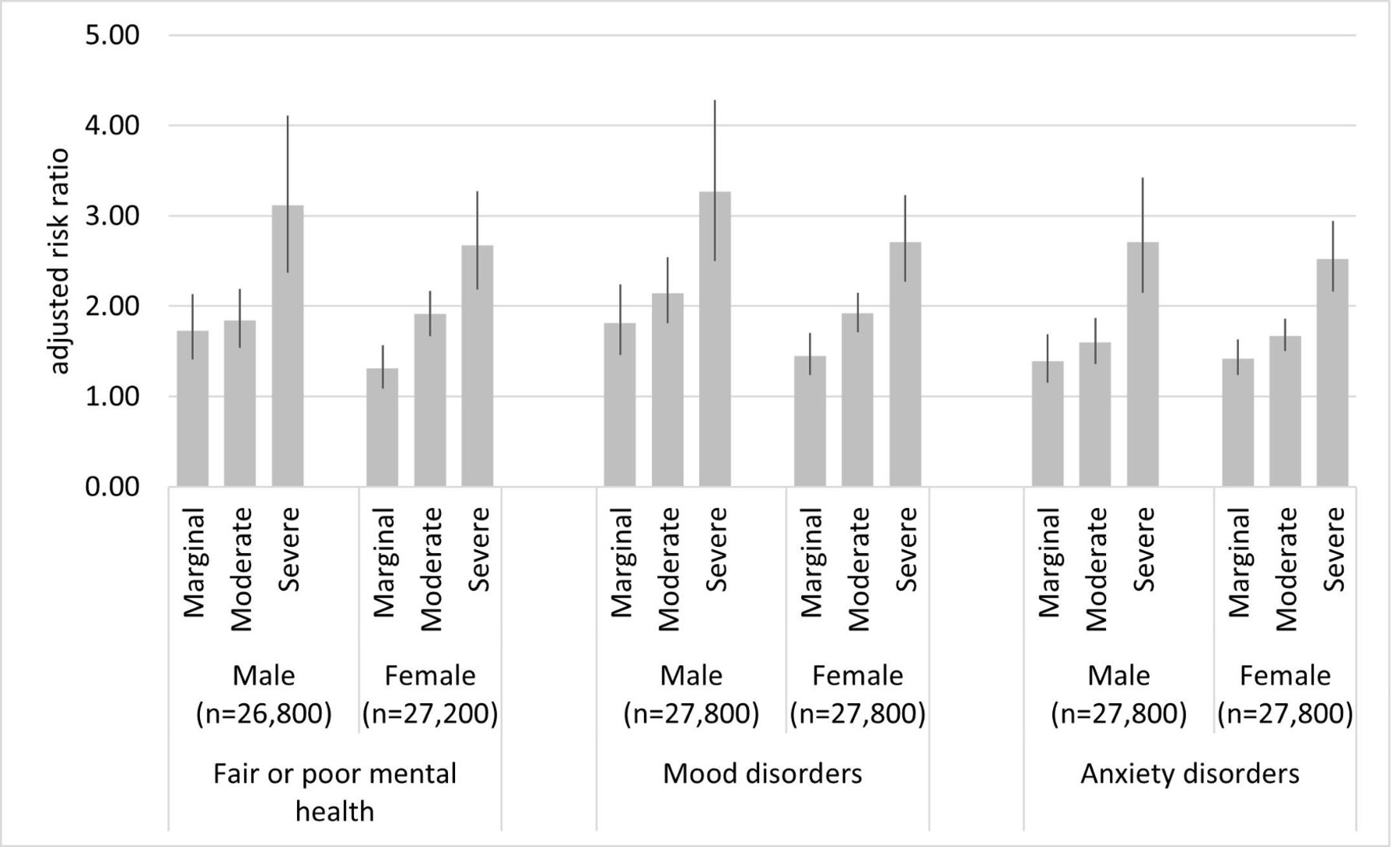
The association between moderate food insecurity and the three nationally measured outcomes (fair or poor mental health, mood disorders, anxiety disorders) was stronger among young adults than among adolescents (p<0.05 for all interactions; figure 2). Severe food insecurity was more strongly associated with fair or poor mental health among young adults than among adolescents (interaction p<0.001). The association between marginal food insecurity and fair or poor mental health was weaker for females than for males (interaction p<0.05; figure 3). Compared with cycle 2011–2012, the association between marginal food insecurity and anxiety disorder was weaker in 2017–2018 (interaction p<0.01; online supplemental eFigure 2).

Poorer mental health associated with food insecurity, by age group. Data show risk ratios of marginal, moderate and severe food insecurity on three binary outcomes of self-reported mental health problems among adolescents 12–17 years old and young adults 18–24 years old, adjusting for socioeconomic confounders. Reference group is food-secure youth.
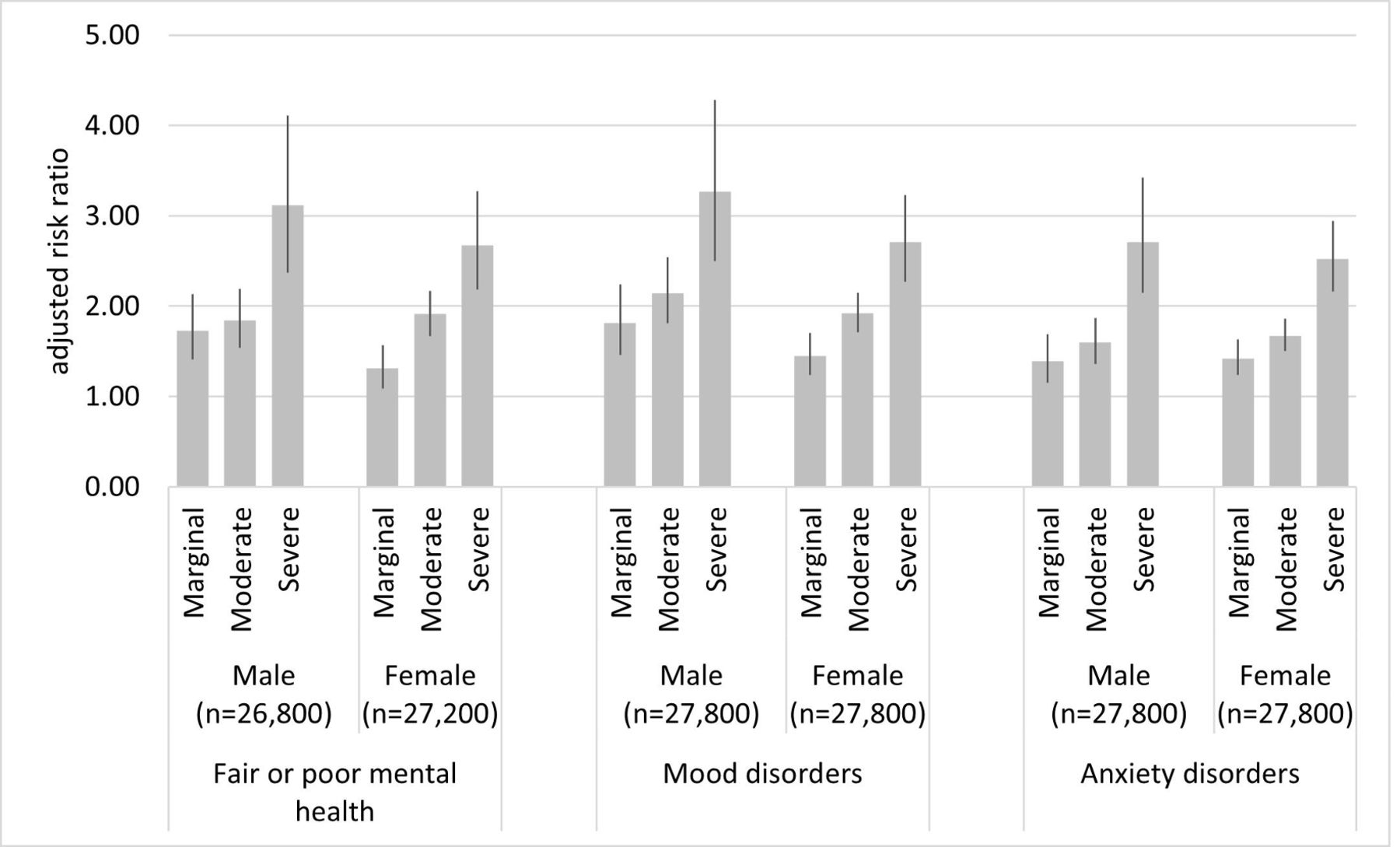
Poorer mental health associated with food insecurity, by gender group. Data are risk ratios of marginal, moderate and severe food insecurity on three binary outcomes of self-reported mental health problems among male and female youth 12–24 years old, adjusting for socioeconomic confounders. Reference group is food-secure youth.
Sensitivity tests on alternate thresholds for distress and depression yielded results consistent with those from the primary analyses (online supplemental eTable 5). We also obtained qualitatively similar results to those from the main analyses when fitting linear models on logged forms of distress and depression outcomes or removing Nunavut from the sample.
We estimated average predicted probabilities of reporting mental health issues based on the adjusted models from primary analyses (figure 4; online supplemental eTable 6). Consistent with our regression estimates, a graded, dose–response pattern was found for all outcomes, with those in more severe food insecurity having progressively more mental illness. Of all the outcomes analysed, distress was most likely to be experienced, with the adjusted probability ranging from 17.3% if food-secure to 39.0% if severely food-insecure. Suicidal ideation was the least likely outcome, with probabilities of 0.8% to 5.4%. The other outcomes’ probabilities ranged between 4.6% and 17.8%. Young adults had higher probabilities of reporting negative mental health outcomes than adolescents regardless of one’s food insecurity status. Females and respondents from more recent survey cycles presented generally higher probability of experiencing poorer mental health outcomes than their male and earlier-cycle counterparts, respectively, though some differences were not statistically significant.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Food-insecure youth show higher probability of mental health problems compared with food-secure youth. Data are adjusted average predicted probability of six binary outcomes of mental health problems by food insecurity status among youth 12–24 years old, estimated from fully adjusted Poisson models on overall youth sample.
Discussion
Drawing data from a large population-based sample of Canadian youth, we found that household food insecurity is significantly associated with several mental illnesses in youth after adjusting for income and other sociodemographic characteristics. A graded, dose–response association was found in all outcomes, with more severe food insecurity predicting greater risk. The association between moderate food insecurity and self-reported mental health issues was stronger among young adults than adolescents.
This study is among the first to establish the adjusted association between a validated household food insecurity scale and multiple measures of youth mental health in Canada. The findings are consistent with prior studies,3 4 14–25 confirming the hypothesised co-occurrence of food insecurity and poor mental health. Longitudinal research may examine whether negative outcomes observed in food-insecure adults, such as suicide,31 stem from food hardship and related stressors during adolescence. While more severe food insecurity may impact youth mental health through pervasive material deprivation, poor food quality and nutrient inadequacy, our findings reveal that even mild food insecurity coincides with higher risks of mental disorders, possibly due to chronic distress related to food hardship.12 That food insecurity is linked to mental health independently of household income supports the hypothesis that food insecurity is a more direct measure of low financial resource, encompassing risk factors beyond low income such as high living cost, poor nutrition, stigma and marginalisation.32 Although income is a powerful predictor of food insecurity, the overlap between food-insecure households and those in or near poverty is far from perfect.33 Food insecurity is essentially distinct from income in its relationship with mental health, commanding different sociocultural interpretations than poverty per se. Food insecurity may be a common and salient source of anxiety in the household.
These results are in line with the previously reported link between social and psychological dimensions of poverty among adolescents in higher-income countries,34 suggesting that food insecurity indicates social disorganisation and risk in the home environment that are beyond income inadequacy. Socioeconomically disadvantaged youth have poorer access to psychologists and general practitioners than their more advantaged counterparts.9 Lack of access to outpatient mental health services may partly explain why, in the Canadian context of universal healthcare, youth’s emergency department visits and hospitalisations due to mental disorders have increased by 75% and 65% from 2006 to 2018, respectively.35 While household income was adjusted in our analyses, we could not fully control for affordability of drugs or treatments. Future research should examine accessibility to mental health counselling and psychiatric medications in relation to food insecurity among youth.
That food insecurity was more closely associated with mental health problems in young adults compared with adolescents suggests that adolescents are better shielded from food hardships and related stressors by their parents.36 In addition, mental health counselling for children under 18 is covered by Canada’s universal healthcare but substantial out-of-pocket expenses are required for adults seeking the same service.37 The affordability issue—not fully accounted for by the income control—may expose young adults to greater risk of mental health crises than adolescents. Moreover, since many young adults have just begun living away from their parents or become parents themselves, the economic and health circumstances they face are fundamentally distinct from those of adolescents. Although we controlled household and individual differences in our analyses, there were likely unobserved differences between age groups such as differing risks of mental problems and reporting bias.27
The co-occurrence of mental illnesses and food insecurity points to the importance of coordinated policy intervention that tackles both issues. Policymakers and health practitioners should recognise food insecurity as a risk factor of mental illness during the formative stage of youth development, especially during the transition to adulthood. Effective interventions to improve food security and mental health in this population will benefit their well-being into later adulthood.7 15 24 25 Besides the overlap with low income, food insecurity may also intersect with non-financial deprivations such as neglect and family dysfunction with profound consequences for youth’s psychological well-being. Our results showed that links between food insecurity and youth mental health were not specific to any demographic subgroup examined. The increasing prevalence in mental illnesses over time poses an imminent threat to the well-being of all youth,5 and COVID-19 and the consequent food security crisis may exacerbate the impact of mental illnesses for the most vulnerable ones.38
Our findings further point to the need for effective interventions to address food insecurity, and particularly severe food insecurity, among families with youth. Families with underage children and young adults face higher than average food insecurity risk in Canada.1 2 Cash transfers like the Canada Child Benefit have shown success in reducing severe food insecurity among Canadian children under 1839 even though strengthening food security was not a goal of the programme. Similar policies that increase financial resources to low-income households are associated with lower food insecurity among US families with children,40 though in-kind transfers like school meals and food stamps do not currently apply to Canada and their potential effects on food insecurity in this country would largely depend on programme uptake among other factors.41 Young adults’ food insecurity warrants more research attention.
Young adults, unlike adolescents, are transitioning towards economic independence and their exposure to risk of food insecurity hinges on a more complex set of personal and environmental determinants including employment, schooling, parenting and social assistance. More research is needed to examine the effects of income-based interventions and support programmes on youth’s food insecurity. Strengthening food security at young ages may have long-term health benefits.42 Mental health problems, if not addressed early, heighten risk of food insecurity and more severe mental health challenges in late adulthood. Health providers and policymakers must foster initiatives to systematically address food insecurity to minimise its harm on youth.
Limitations
Our findings should be interpreted in light of some limitations in our analysis. First, we could not rule out the possibility of reverse causality and omitted variable bias despite our efforts to establish food insecurity as an upstream determinant of health. That said, the observed dose–response relationships between food insecurity and most outcomes corroborate existing evidence in approximating causality. Longitudinal data that trace individuals’ food insecurity status and health outcomes over time would help determine the prospective association between early-life food insecurity and subsequent mental health. Second, adolescent interviewees 16–17 years old answered food insecurity questions in CCHS 2007–2008 but not later. The methodological inconsistency may bias our estimates in undetermined direction and warrants further study. Third, distress, depression and suicidal ideation were measured in select jurisdictions and years, limiting the generalisability of our estimates and detail level of our analysis. Future studies may seek nationally representative data to validate our findings. Fourth, our three mandatory outcomes were built from single questions; however, the convergence of their estimates with those of optional outcomes helped reassure their validity. Fifth, young adults living independently may be more susceptible to mental problems than their peers living with parents due to financial difficulties. Moreover, life events such as parental unemployment, divorce and disability may contribute to various adversities among youth, including food insecurity and mental problems. Since CCHS does not collect data on those factors, we acknowledge it as a limitation and call for their exploration using other datasets. Last, our study focused on the economic struggle even though food insecurity and mental health are both multidimensional. Research is warranted to explore the interaction between non-economic aspects of food insecurity and mental health.
Conclusion
Our study marks an important step towards understanding the relationship between household food insecurity status and youth’s mental health. Youth from food-insecure households are more likely to experience negative mental health outcomes than their food-secure counterparts, especially among young adults. Effective policies are needed to reduce household food insecurity, strengthen youth’s mental health and promote health equity.
What is already known on this subject
Food insecurity is a risk factor for mental illnesses, which are rising among youth worldwide.
Few studies have examined mental health by severity of food insecurity among Canadian youth.
Little is known about the demographic heterogeneity in such associations.
What this study adds
Household food insecurity has a dose–response association with mental health problems among Canadian youth.
The association is stronger for young adults than adolescents but similar between gender groups and over the 2007–2018 period.
Policies reducing household food insecurity may support youth mental health.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are accessible through Statistics Canada with restrictions. For the present study, the data were accessed under contract through the Statistics Canada Research Data Centre at the University of Toronto.
Ethics statements
Acknowledgments
This research was conducted at RDC Toronto, a part of the Canadian Research Data Centre Network (CRDCN). This service is provided through the support of the University of Toronto, the Canadian Foundation for Innovation, the Canadian Institutes of Health Research, the Social Science and Humanity Research Council, and Statistics Canada. We thank Joannah and Brian Lawson Centre for Child Nutrition at the University of Toronto and Canadian Institutes of Health Research (grants PJT-153260 and PJT-165971) for their funding.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrFMen
Contributors FM and VT designed research. FM and FE conducted research. FM analysed data. FM, VT and FE wrote the paper. FM had primary responsibility for final content. All authors read and approved the final manuscript.
Funding This work was supported by Joannah and Brian Lawson Centre for Child Nutrition at the University of Toronto (no grant number assigned) and Canadian Institutes of Health Research (grants PJT-153260 and PJT-165971).
Disclaimer The funder had no role in the design and conduct of the study; collection, analysis, and interpretation of data; writing of the article; or decision to submit the article for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.