Article Text

Abstract
Background Real-world evaluations of complex interventions are scarce. We evaluated the effect of the Salut Programme, a universal child health promotion intervention in northern Sweden, on income-related inequalities in positive birth outcomes and healthcare utilisation up to 2 years after delivery.
Methods Using the mother’s place of residence at delivery, the child and the mother were classified as belonging to either the control area (received care-as-usual) or the intervention area (where the intervention was implemented from 2006) and either the premeasure (children born between 2002 and 2004) or the postmeasure (children born between 2006 and 2008) period. Parents’ earned income was used as the socioeconomic ranking variable. The Relative Concentration Index was computed for six binary birth outcome indicators and for inpatient and day patient care for children and their mothers. Changes in inequality over time were compared using a difference-in-difference approach.
Results Income-related inequalities in birth outcomes and child healthcare utilisation were absent, except that full-term pregnancies were concentrated among the poor at premeasure in the intervention area. In contrast, mothers’ healthcare utilisation was significantly pro-poor in the control area. The extent of inequality changed differentially between premeasure and postmeasure for two birth outcomes: full-term pregnancies and infants with normal birth weight. Inequalities in healthcare utilisation did not change significantly in either area over time.
Conclusion In northern Sweden, income-related inequalities in birth outcomes and child healthcare utilisation are largely absent. However, relative inequalities in mothers’ healthcare utilisation are large. We found no evidence that the Salut Programme affected changes in inequality over time.
- public health
- health promotion
- income
- pregnancy outcome
- registries
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
BACKGROUND
Reducing health inequalities has become a major societal concern.1 Health is conceptualised as a form of human capital, and improving the health of disadvantaged children is promoted to combat lifelong health inequalities.2 3 Development prenatally, during infancy and childhood influences lifelong health.4–8 Early years are the most sensitive period when exposure to inequality is strongly related to health later in life.9
Children in Sweden are generally healthy, yet health inequalities exist between different segments of the population.10 Differences in parental education, occupation and income are related to differences in child health outcomes and life expectancy.11 For example, children from disadvantaged families had 131% higher risk of mortality, 40% higher risk of hospitalisation and 38% higher risk of mental illness compared with children from better-off families.12 The Swedish Commission for Equity in Health has highlighted the need to provide equal opportunities in different sectors of society, with a focus on the most disadvantaged groups.11 13 14
There is a general understanding that targetted programmes are required to reduce inequalities and that universal health promotion interventions particularly benefit wealthy families. Some attempts have been made to evaluate comprehensive strategies to combat inequalities, most notably in England.15 However, we are aware of few published evaluations of the equity impact of universal public health interventions.
The Salut Child Health Intervention Programme is a universal health promotion intervention targeting all expectant parents and children in the region of Västerbotten in northern Sweden.16 Results from a recent study suggested that the Programme is effective in improving average health outcomes at birth at lower costs than care-as-usual; thus it could be good value for money.17 We aimed to contribute to the evidence on the equity impact of universal health promotion programmes by investigating the effect of the Salut Programme on income-related inequalities in birth outcomes and healthcare utilisation for children and mothers during the first two years after delivery.
METHODS
The Salut Programme
In Sweden, antenatal care and child healthcare are free of charge and attended by almost everyone. The Salut Programme, initiated in 2005, is integrated within ordinary healthcare in the region of Västerbotten in northern Sweden.16 18–20 The Programme has a multisectorial and family-centred approach to health promotion that targets all expectant parents and children. The name ‘Salut’ originates from the term ‘salutogenesis’, which highlights the individual’s capacity and resources to generate health.21
Study design and study population
The stepwise implementation of the Salut Programme created a natural experiment, and the availability of register data enabled a retrospective observational study design.22 We compared birth outcomes and healthcare utilisation between geographical areas where the Programme was implemented from 2006 (intervention area) with the remaining part of the region (control area). We included all children born between 2002 and 2004 (before the Programme was implemented anywhere) and their mothers, defined as the premeasure period. Accordingly, we included all children born between 2006 and 2008 (after the Programme was implemented in some areas) and their mothers, defined as the postmeasure period. Thus, four study groups were formed: intervention-pre, intervention-post, control-pre and control-post.
Outcomes and socioeconomic status
Outcome measures were described in detail in an earlier evaluation.17 We selected measures that could potentially capture the effect of the Programme on the health of mothers and their children. Birth outcome indicators were coded to measure good health, in order to correspond with the Programme’s design as a wide-ranging, health-promoting intervention. Healthcare utilisation measures were also included. The outcomes are fully defined and summarised in table 1.
Sample averages for income, birth outcomes and healthcare utilisation divided into intervention and control areas and premeasure and postmeasure periods, respectively
Childbirth outcomes (binary indicators): full-term pregnancy; vaginal delivery; normal birth weight; normal weight for gestational age; normal Apgar score (at 5 min); child healthy at discharge.
Child’s healthcare utilisation: inpatient care within 2 months after birth (binary); inpatient care within 2 years after birth (cumulative number of days); day patient care within 2 years after birth (cumulative number of visits).
Mother’s healthcare utilisation: inpatient care related to delivery (cumulative number of days); inpatient care excluding delivery within 2 years after child’s birth (cumulative number of days); day patient care within 2 years after child’s birth (cumulative number of visits).
Our focus was the distribution of these outcome measures across the income distribution, referred to here as ‘income-related health inequality’. We measured income as the sum of earned income for the child’s parents in the year of birth. To abstract from differences between groups due to inflation, nominal incomes were adjusted to a common reporting year (2008) using the Consumer Price Index.23
Statistical analysis
Descriptive statistics were computed for parental income quintiles; birth outcomes; and the healthcare utilisation measures, in the intervention and control areas for the premeasure and post-measure periods, respectively.
The Relative Concentration Index (RCI) was used as a measure of inequality. The RCI is a summary measure that ranges from −1 to +1. If there are no income inequalities in the distribution of the outcome variable, the RCI equals zero. A negative value indicates that the outcome variable is concentrated among the poor, and a positive value indicates the opposite. We used the RCI because we wanted to relate the main findings to how large the inequality was in absolute terms.24 The Absolute Concentration Index (ACI), which relates the extent of inequality to the mean value of the outcome variable,25 was therefore computed for those variables for which there was a significant degree of relative inequality. Index values were computed using the convenient regression method implemented in the conindex Stata routine.26
The analysis was carried out in three main steps. First, for each outcome, we assessed whether there was a significant degree of income-related inequality. The RCI values for each outcome, in each area and time period, were plotted.27 Second, we used F-tests to examine whether the RCI within each area changed from premeasure to postmeasure. Third, we assumed normality and used a z-test to assess whether the change within the intervention area over time was different from the change within the control area over time (represented by the difference-in-difference concentration index). P values less than 0.05 were used to determine statistical significance.
Finally, we plotted concentration curves (CC) for those outcomes for which the RCI was significantly different from zero in at least one area and one time period. CCs reveal whether any pro-poor or pro-rich patterns are constant across the income distribution. In the CC, the cumulative proportion of the outcome is ordered from lowest to highest (eg, 0–100% of all child inpatient days) and plotted against the cumulative proportion of the population ranked from the poorest to the richest.25 If the CC lies on the diagonal, there are no income inequalities in the distribution of the outcome. If the CC lies above the diagonal, the outcome is more concentrated among the poor. If the CC lies below the diagonal, it indicates the opposite.
RESULTS
Characteristics of the participants
The number of newborns in Västerbotten was about 7700 in the premeasure period (2002–2004) and about 7000 in the postmeasure period (2006–2008). Of these, 888 children and their mothers were considered to be exposed to the Salut Programme because the children were born in the intervention area during the postmeasure period (‘intervention-post’). Details are given in table 1 and shortly commented on below.
Intervention area families were poorer on average, and the difference in median income across quintiles was bigger than in the control area. In both areas, the median income in the lowest quintile decreased from premeasure to postmeasure, but increased in all other quintiles.
Most children (78–99% depending on indicator) had positive birth outcomes. The proportion of children readmitted to the hospital during the first 2 months after birth decreased from 7% at premeasure to 4% at postmeasure. The average duration of the mother’s inpatient care related to delivery decreased by one half-day. In the 2 years after delivery, the mean cumulative duration of inpatient care was 1.4–1.9 days for children and 0.4–0.5 days for mothers. Results of our previous study suggested that the intervention contributed to an improvement in average outcomes and a reduction in healthcare costs.17
The extent of relative inequality
Results regarding income-related inequalities are summarised in figure 1 for positive birth outcomes and in figure 2 for healthcare utilisation. Arrows indicate changes in the RCI over time (premeasure to postmeasure) within each area. The RCI values, SEs and statistical tests for whether changes over time differed between the areas are provided in the online supplementary material tables AI and AII.
Supplemental material

Relative income-related inequalities in positive birth outcomes for children.

Relative income-related inequalities in healthcare utilisation.
Positive birth outcomes for children were mostly equitably distributed (figure 1). The exception was full-term pregnancies in the intervention area at premeasure, which were concentrated among the poor to a small but statistically significant extent (RCI −0.019, p=0.001) (online supplementary material table AI).
Children’s healthcare utilisation was equitably distributed (figure 2). None of the RCIs was significantly different from zero (online supplementary material table AII). In contrast, mothers’ healthcare utilisation was significantly pro-poor in the control area, especially at postmeasure (figure 2). The magnitude of inequality was small for delivery-related inpatient care (RCI −0.014, p=0.014), but large for other inpatient care (RCI −0.145, p=0.050 at premeasure; RCI −0.295, p=0.000 at postmeasure) and for day patient care at postmeasure (RCI −0.145, p=0.027) (online supplementary material table AII).
Changes in relative inequality pre- to post-measure
Arrows in figure 1 indicate that the extent of inequality changed over time for two birth outcomes: full-term pregnancies and normal weight for gestational age. In the former case, changes in inequality over time differed between the two areas. In the intervention area, the pro-poor concentration of full-term pregnancies at premeasure disappeared at postmeasure (F-stat 7.4, p=0.007). In the control area, full-term pregnancies were equitably distributed at both premeasure and postmeasure. In other words, the intervention area became more similar to the control area over time (difference-in-difference RCI 0.0206, p=0.003; online supplementary material table AI). The second arrow in figure 1 indicates that although none of the RCI values for normal birth weight for gestational age was significantly different from zero, this outcome became significantly more concentrated among the poor in the control area over time (F-stat 5.50, p=0.019). However, the two areas did not differ significantly from each other in terms of changes in inequality between premeasure and postmeasure (difference-in-difference RCI −0.0004, p=0.96). As indicated by the lack of arrows in figure 2, the extent of inequality in healthcare utilisation did not change significantly over time in either area (online supplementary material table AII).
Concentration curves
We plotted CCs for the four outcomes for which the RCI was non-zero in at least one time period in one area. CCs for full-term pregnancy and mother’s inpatient care related to delivery closely followed the diagonal (online supplementary material figures AI–AIV). CCs for mother’s inpatient care (excluding delivery) in the intervention area approximately followed the diagonal at premeasure, but had a subtle inverse s-shape postmeasure, from pro-poor among the poorest to pro-rich among the richest (figure 3). The corresponding control area CCs lay more consistently above the diagonal, indicating a pro-poor concentration across the income spectrum (figure 4). CCs for mother’s day patient care were strongly jagged in the intervention area, reflecting the small number of women who had day patient care (online supplementary material figure AV), while control area CCs were located above the diagonal (online supplementary material figure VI).
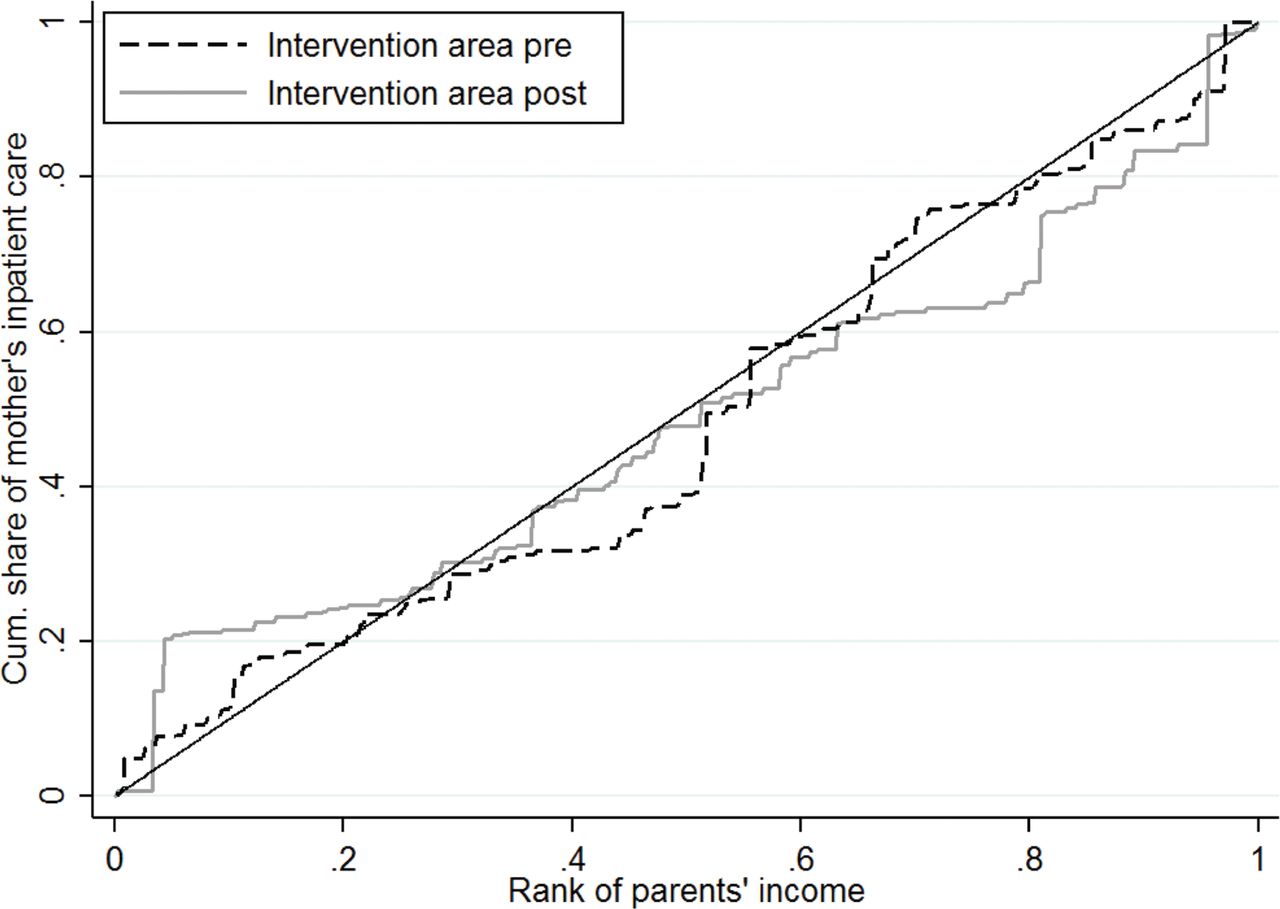
Intervention area concentration curves for mother’s inpatient care in the first 2 years after delivery (excluding delivery).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Control area concentration curves for mother’s inpatient care in the first 2 years after delivery (excluding delivery).
The extent of absolute inequality
Finally, we computed ACIs for mother’s healthcare utilisation (online supplementary material table AIII). The ACI values in the four cases with a significant degree of inequality, all in the control area, were: −0.04 days (p=0.014) for inpatient care related to delivery at postmeasure; −0.07 days (p=0.050) at premeasure and −0.13 days (p=0.000) at postmeasure for inpatient care unrelated to delivery; and −0.002 day patient visits (p=0.027) at postmeasure. Thus, income-related inequalities in utilisation were small in absolute terms.
DISCUSSION
Summary of main findings
In this study, we found surprisingly few income-related inequalities in positive birth outcomes or child healthcare utilisation within 2 years after birth. In contrast, mothers’ healthcare utilisation after delivery was significantly concentrated among the poor in the control area, though not in the intervention area. Furthermore, we found that the size of the relative inequalities was large for the mother’s inpatient care unrelated to delivery and day patient care. In absolute terms, however, these inequalities were small.
Our analyses suggest the Salut Programme had no effect on income-related inequalities in either birth outcomes or healthcare utilisation. The extent of inequality mostly did not change from premeasure to postmeasure. In one case, the intervention area became more similar to the control area, in what can be interpreted as a negative development: a pro-poor concentration of a positive birth outcome (full-term pregnancies) disappeared.
Comparison with other studies
Our results regarding birth outcomes contradict those in a 2016 report by the Swedish National Board of Health and Welfare that found that mother’s educational level was strongly correlated with perinatal death, low 5-min Apgar score, child being small for gestational age, premature birth and elective caesarian section, also after controlling for risk factors such as mother’s country of birth, age and smoking.28 Two main reasons may explain the difference in findings. First, it is well known that income-related and education-related health inequalities do not necessarily display the same trends. In Sweden, the focus in public debate and research has been on education-related inequalities; however, income is nowadays receiving more interest.29 Internationally, multidimensional methods have recently been proposed that include both income and education and leave the choice of relevant socioeconomic variable to the reader.30 Nevertheless, arguments for choosing income include the view that it is more strongly associated with mortality than education or, say, occupation,31 and that policy-makers are becoming familiar with the concentration index, which is suited for continuous variables, such as income.
Second, we coded the binary birth outcome variables so as to indicate positive outcomes rather than ill-health, and evaluated the Salut Programme for its effect on relative inequality in these ‘attainments’. Thus, our analysis involved several normative value judgements, and alternative judgements would have led to different methodological choices, and thereby possibly different conclusions. Specifically, no relative measure satisfies the mirror property, that is, that the magnitude of inequality would be the same regardless of whether attainments or ill-health levels are measured.32
Strengths and limitations
To answer our main research question, whether the Salut Programme had an effect on health inequalities, we computed a difference-in-difference RCI, which to our knowledge is an innovative approach. Our approach breaks down the overall question into three: whether outcomes are unequally distributed with respect to income (ie, whether inequality exists); whether inequality is changing over time; and whether those changes have been affected by the intervention. In practice, the latter questions were only relevant for mothers, because child outcomes were mostly equitably distributed.
Our choice of inequality measure was informed by our view that national policy-makers are more familiar with the RCI and CC than alternative methods. Inequality in mothers’ healthcare utilisation appeared to vary across the income distribution. Since such variation is not captured by the RCI, we used CCs to complement the analysis. However, we relied on the RCI as a summary measure to draw conclusions about the equity impact of the intervention.
Our interpretation is that in the Swedish context, relative inequality is an overriding concern; however, decision-makers expect absolute inequality to be presented alongside the relative as complementary information. For this reason, we used the RCI rather than one of the 'corrected' concentration indices proposed in the literature. A resulting limitation was that the range of the RCI for the binary health outcomes became very small, because the range depends on the mean, which was close to one in our data.
Policy implications
An increasing body of evidence suggests that an equal distribution of health benefits the population as a whole.14 However, there are concerns that participation in universal health promotion programmes, such as the Salut Programme, differs by socioeconomic status. An intervention that is intended to improve health in the overall population may widen inequalities if its benefits are concentrated among the better-off.33 It is therefore imperative that such programmes are evaluated from an equity perspective. Our result that the intervention did not increase inequalities is, therefore, an important finding.
In Swedish public health discourse, the unequal distribution of health between and within different groups is considered a problem, and public health stakeholders at national, regional and local levels are seeking more knowledge of how different interventions affect population health.34 There are surprisingly few examples of population-based real-world interventions that have been shown to reduce health inequalities. While our study does not provide evidence of what works to reduce inequalities, our view is that evidence of no inequality effects is equally important.
In Sweden, increasing income inequality over time highlights the need to examine whether income-related health inequalities are also increasing. The Gini Index rose from 25.3 in 2003 to 29.2 in 2015.23 The difference in median income between the highest and lowest quintiles in our data is smaller than in the Swedish population as a whole. This is likely because income drops temporarily during parental leave, more so in absolute terms among high-income earners. As in other countries, Swedish political parties differ in terms of policy regarding income inequalities. In contrast, parties across the political spectrum agree on the undesirability of low educational attainment. Thus, reaching consensus on how to respond to income-related health inequalities is likely even more difficult than for education-related health inequalities.
CONCLUSION
In northern Sweden, positive birth outcomes and child healthcare utilisation in the 2 years after birth are equally distributed with respect to income, but relative inequalities in mother’s healthcare utilisation are large. We found no evidence that the Salut Programme had any effect on changes in inequality, neither positive nor negative.
What is already known on this subject
Reducing health inequalities is a common health policy aim. However, few interventions are explicitly evaluated for their impact on health inequalities. As a result, little is known about whether universal health promotion interventions are good or bad for equity.
What this study adds
We find no evidence that the Salut Programme, a universal child health promotion programme in northern Sweden, affected inequalities in birth outcomes or in healthcare use after delivery. The Salut Programme is now a rare example of a routine practice intervention for which there is evidence of impact on average health, cost-effectiveness and health inequalities.
Policy implications
Universal child health promotion may be supported as a relatively cheap and, as in the case of the Salut Programme, an effective approach to improving average health. We find that while its universal, salutogenic approach is unlikely to aggravate health inequalities, other approaches are required to address them.
Acknowledgments
We thank Per E. Gustafsson from Norrland Observatory for Equity in Health and Health Care for comments at an early stage of this work. Discussants and participants at the following conferences and workshops gave suggestions that allowed us to further improve the work: Third workshop of the Nordic Network for Health Policy, Health Management and Health Services Research (Uppsala 2019), Umeå SIMSAM Lab workshop (Umeå 2019), International Health Economics Association Congress (Basel 2019), European Public Health Conference (Marseille 2019).
REFERENCES
Footnotes
Contributors A−MP-B, ML and IF conceived and designed the work. AI acquired the data as the principal investigator for the Umeå SIMSAM Lab. JH prepared the data for analysis. A−MP-B, ML and JH analysed the data. A−MP-B lead the interpretation of the results and drafting of the manuscript. ML, EE, JH, AI, FS and IF contributed to the interpretation of results and drafting of the manuscript. A−MP-B, AI and IF made substantial critical revisions to the manuscript. All authors approved the final version. A−MP-B is responsible for the overall content as guarantor.
Funding This work was supported by the Swedish Research Council for Health, Working Life and Welfare (FORTE) grant number 2017-00912. The Umeå SIMSAM Lab data infrastructure used in this study was developed with support from the Swedish Research Council and by strategic funds from Umeå University.
Competing interests None declared.
Patient consent for publication The study used register data, and therefore the question of patient consent was not applicable.
Ethics approval The Regional Ethical Review Board in Umeå gave clearance for the Salut Programme research (2010-63-31M) and for the Umeå SIMSAM Lab research (2010-157-31Ö).
Data sharing statement Data may be obtained from a third party and are not publicly available. This study used data from the Umeå SIMSAM Lab. Access is restricted to a secure data Lab, and data cannot be removed from the Lab. Further information about data access is available at: www.simsam.org.umu.se.
Provenance and peer review Not commissioned; externally peer review.ed